For me, as a child, contentment arrived in the form of a pencil and paper. I drew pictures throughout my childhood. I continued to draw occasionally through college, but time limitations and other commitments led to a nearly 10-to-15-year post-grad absence from drawing. One afternoon while sitting on the porch with my family, I noticed a petunia had fallen onto the table from a hanging basket. I had a pencil nearby, so I picked it up and began to sketch. I noticed at first it was challenging to create an accurate representation of the contours and contrast of the flower petals, but gradually I was able to get back in the ‘zone.’ I shared my drawing with my family and heard myself describing how I translated my vision of the petunia to paper. It was this ability to connect with others through art in a unique, relatable way that made it so rewarding, and I was motivated to continue engaging with this familiar creative process.
Bridging Art With DPT Instruction
In my experience, I have also seen how art can have a substantial impact on the viewer in several ways, from drawing out various emotions to creating a means for deeper discussion or understanding. Hence, I set out to explore ways to bridge art with my current role as a core faculty member in a Doctor of Physical Therapy (DPT) program. In my quest for bringing art into my professional life, I thought about the physical therapy (PT) profession and some of the aspects that make it unique from other health disciplines. One concept that stood out was the many ways physical touch, or tactile perception, are utilized when performing the duties in PT. I decided to direct my art to the concept of physical touch as a foundation of trust between the patient and clinician.

Illustrating Trust Through Touch
In formulating ideas to illustrate the construct of trust through physical touch and the nuances of physical touch in PT practice, one scenario stood out. In this image that I created (Figure), the clinician provides light hand hold while the patient maintains a single limb stance—communicating the idea that trust is an extension of physical touch, and vice versa. The physical therapist’s open hand with light touch demonstrates warmth and confidence in the patient while still being available to physically support the patient if needed.
In order to interpret the subtle changes in a patient’s response during a dynamic clinical scenario such as this, one must appreciate the nuances, intent, and value of physical touch in this context. During this intervention, the patient trusts the prescribed exercise will help them reach their goals in a manner that maximizes benefits while simultaneously minimizing risk. By varying the amount of touch during the intervention, it displays the physical therapist’s confidence and trust in the patient as the patient gains independence as part of the rehabilitation process. The decision-making process of when and how to use physical touch during patient care is an important learned skill, and this drawing helps to encourage clinicians or students to consider its application and desired outcome.
Formulating the Image
I recall that as I was completing this drawing, there were several decisions that needed to be made. Initially, I was going to provide a detailed representation of the hands only, while leaving the other objects vaguer (gait belt, clothing, etc.), as I thought: 1) a focus specifically on the aspect of physical touch would resonate differently with the viewer, and 2) I had never drawn clothing in great detail before! The clothing, although somewhat technically difficult, became one of my favorite aspects of the drawing, as it adds a layer of texture and movement that otherwise would have been absent. This decision, and the reward it produced, adds motivation to take more risks during the creative process in the future.
Although I have never sculpted, the process of charcoal drawing, blending, and removing/adding contrast makes me think there are some similarities with sculpting. There were parts of the drawing that initially did not turn out how I had intended, but the ability to modify and ‘sculpt’ certain parts of the drawing allowed flexibility to take certain creative risks to a degree. One example, again, was the clothing. The pants were initially quite dark throughout, which made it difficult to discern and appreciate the details of the folds/tension of the fabric. I decided to lighten the fabric by removing some of the charcoal with the intent to allow the viewer to notice the position of the lower extremities with greater ease. This flexibility that accompanies charcoal drawing is one aspect that makes it an enjoyable medium to use in this way.
Visible Thinking
To better appreciate how this artwork might inform one’s teaching/practice, I met with several DPT students to garner their perspective. We met virtually as a small group and went through the Visible Thinking process of ‘See, Think, Wonder’ from Harvard University.1 This strategy encourages students to carefully observe what is in front of them, make thoughtful interpretations and express their viewpoints, and create a sense of curiosity and inquiry.
Among medical learners, the use of visual thinking strategies may improve several attributes relevant to clinical practice, including our skills in observation, interpretation, and critical thinking;2-5 tolerance for ambiguity;6 fostering of empathy;6 and development of a sense of wonder.7 Developing wonder among medical students has been promoted due to its several potential benefits, such as fostering the delivery of humanistic patient care, developing a commitment to lifelong learning, and encouraging innovation.7,8
Student Insights
After a brief period of quiet viewing, the students discussed their observations of the artwork. The first theme that emerged was the notion of helping (from the physical therapist), but also trusting and allowing the patient to use assistance as needed. This concept was further explored by the supportive hand hold; the patient wearing a gait belt, but it’s not being used for support by the physical therapist; and the positioning of the physical therapist in front of the patient versus directly to the side or behind. Some felt the scenario reminded them of a dance, where one partner would lead while the other followed.
The concept of trust was mentioned on several occasions, even without the students knowing the title of the artwork. The students also pointed to the lack of facial cues and having to rely on the patient’s body posture to appreciate various qualities of this task. Was this task challenging? Enjoyable? Engaging? Hearing reflections through the lenses of DPT students helps to inform my teaching by encouraging me to adapt based on their current level of understanding, and how their questions or perspectives may evolve over time as they are introduced to diagnoses, rehabilitation techniques, and experiences from clinical education.
One aspect of the artwork that was noticed among the students is the lack of a visual background or setting for this patient-clinician encounter. Honestly, there was not much intentionality behind this, but as I spent more time with the drawing and hearing the student feedback, I believe this allows the viewer to imagine this scenario occurring in a variety of settings (outpatient, hospital, etc.), so the viewer is not limited in their interpretation by setting alone. The lack of background, along with other features in the drawing, may contribute to the sense of wonder and its relevance to clinical practice as discussed earlier.
Clinical Questions
After having time to sit with the drawing, the viewer may begin to question the reason, or diagnosis, for the patient being in PT, and why the patient is specifically performing this task. The viewer scans for clues in the drawing that may help fill in the necessary details to lead them down one diagnostic path versus another. The mystery around the patient’s condition also encourages the viewer to recall various patient presentations discussed in the classroom or observed clinically, in order to develop a working hypothesis when assimilating various pieces of information from the patient’s history and examination. One of the aims of this drawing is to ignite the critical thinking process, which is often threaded throughout DPT curricula.
Conclusion
In conclusion, my reintroduction to drawing has been rewarding on multiple levels, most notably the enhanced ability to connect with others and share ideas. As an educator, artwork allows me to better understand the student perspective through facilitated discussion—offering insight to adapt my teaching practices to meet their learning needs and provide an opportunity for further conversation in clinical reasoning. I am grateful to have found a creative outlet that allows me to explore concepts in clinical practice and education from a different perspective, including the construct of trust through physical touch in physical therapy practice.

![]()
This work is licensed under a Creative Commons Attribution 4.0 International License.
In recent decades, the Western concept of health has evolved past a strictly biomedical model to one that encompasses the entire person. While physical survival might be our most basic need, it alone is not enough to sustain us. The desire to engage, to connect, to live meaningfully, and to create is embedded deep within the human psyche. Therefore, the journey to health also needs to address wellness of mind, heart, and spirit.
Therapeutic recreation is an effective modality for use in physical and psychological recovery. Meaningful leisure activity (ie, activities that require the exertion of mental and/or physical energy) has been shown to be especially important, with the opportunity for individuals to proactively lead the process of engagement.1-2 For adults with spinal cord injury (SCI), participation in active leisure is associated with improved quality of life.3-5
In a thematic analysis of leisure experiences for adults with SCI, Chun and Lee1 found that meaningful engagement in such activities contributes to positive personal transformation in the following ways:
- Providing opportunities to discover unique abilities and hidden potential
- Building companionship and meaningful relationships
- Making sense of traumatic experiences and finding meaning in everyday life
- Generating positive emotions
Compared to able-bodied individuals, however, adults with SCI spend more time in passive leisure such as watching television, which is a less satisfying domain of activity than active leisure.6-8
Virtual art production, which includes photography, is an engaging, meaningful activity known to contribute to physiological and psychological resilience through increased brain function connectivity and reduced stress hormone levels.9-10 To the authors’ knowledge, education in the art of photography has not been previously introduced by rehabilitation centers as therapeutic recreation for adults with SCI.
Creative Photography for Adults With SCI
This article describes the development of a pilot program of educational courses in photographic arts for adults with SCI. Outcomes from the pilot, including correlation with the qualitative themes described by Chun and Lee,1 will also be discussed. (Note: All photographs appearing in this article were taken by graduates of the program.)
Figure 1: Under the City (Photograph by Daniel Alvarez.)

Institutional Context
Rancho Los Amigos National Rehabilitation Center (RLANRC; Rancho in this article), consisting of a Los Angeles County public hospital and associated clinics, provides high-quality, comprehensive care for people with disabilities. The hospital admits 4,000 inpatients, and the clinics conduct 78,000 outpatient visits annually. It is accredited by both the Joint Commission and the Commission on Accreditation of Rehabilitation Facilities (CARF), and has been designated as a Center of Excellence for SCI.
Rancho is also recognized as a leader in the application of world-class neuroscience and neurorehabilitation, and is one of only 14 SCI Model Systems in the United States. Rancho Research Institute (RRI) was established in 1956 to oversee and administer Rancho’s medical research. RRI also offers comprehensive community-based educational programs such as Therapeutic Gardening, Return to Driving, Managing Life With Aphasia, Living Life Poststroke, and psychosocial support programs for people with neurologic disabilities and their families and caregivers. A variety of adaptive fitness classes include Pilates, yoga, Tai Chi, balance/vestibular training, cardio-pump, Zumba, wheelchair sports training and competition, and outside programs such as rock climbing, skiing, and various water sports.
Rancho has been designated as the Patient-Centered Medical Home for SCI in Los Angeles County, providing services to its large, often underserved, population. Approximately 1,900 individuals with SCI are seen at Rancho and RRI annually. Compared to other rehabilitation facilities in the U.S., adults with SCI using the Rancho outpatient services are predominantly Hispanic (68%), have a higher level of disability, and tend to come from economically disadvantaged backgrounds, with 49% covered by Medicaid in 2018.
Program Development
Many Rancho adult outpatients who use a wheelchair also experience poverty and reside in disadvantaged communities where a high incidence of violence occurs. For example, 66% of the students in the first year of the pilot program had been shot or stabbed.11 Financial stress, transportation barriers, and other challenges may preclude them from having the time or resources to experience the full benefits of outpatient therapy.
The intention behind the photography pilot was to create an art program with these individuals and their circumstances in mind. Frequently underserved, this group is an important population for rehabilitation programs to include, especially those studying ways to reduce activity limitations and improve quality of life.
Digital Photography as Creative Outreach
Although Rancho has a long history of providing art education to individuals undergoing rehabilitation, its painting classes are conducted primarily for the pediatric population, ages 14 and younger. In considering how to best adopt such a program for an adolescent and adult population, the project developers decided that digital photography might be a more inclusive creative endeavor as it does not presuppose artistic talent.
Accordingly, the team lead created a proof-of-concept project that was funded by the Los Angeles County Supervisors’ office and Rancho. The four-month program was administered by RRI in 2007 and included six adults over 18 with SCI.
Professional photographer Michael Ziegler was chosen as the instructor, and later, as leader of the pilot program series. Ziegler has 36 years of experience in commercial photography; sports photography; stock photography; and fine art photography, including black-and-white street scenes, landscapes, children, energetic motion studies, abstract shapes and colors, still life, and architecture.
After the successful completion of the proof-of-concept project, the RRI pilot program entitled “Photography as Therapy for Individuals with Spinal Cord Injury” was funded by three Quality of Life project grants (the Craig H. Neilson Foundation in 2014 and 2016, and the Christopher and Dana Reeve Foundation in 2017.) In each of the three program years, adults with SCI were recruited from the Rancho outpatient SCI clinic, SCI support groups, and the community, and asked to enroll in a five-month course.
Figure 2: Tractor Fair (Photograph by William Herrera.)

Description of the Pilot Program
Student Demographics and Course Retention. A majority of the students were male (80%), of Hispanic/Latino origin (64%), and had thoracic spinal injuries. Age range was 22 to 47 years and 40% had some previous experience with art, design, media, or photography. Table 1 shows enrollment numbers across the duration of the pilot program and shows course retention for study participants.
Table 1: Photography Course Enrollment and Completion
| Unique Individuals | 2014 | 2016 | 2017 |
| Enrolled in courses | 18 | 14 | 15 |
| Completed courses | 13 | 12 | 12 |
| Retention rate | 72.2 | 85.7 | 80.0 |
| New students | 18 | 8 | 6 |
| Continuing students | — | 4 | 6 |
Course Overview. Digital cameras were provided for use in home and community environments. By the third year, equipment was upgraded from compact cameras to digital single-lens-reflex cameras (e.g. Canon EOS). Students were allowed to keep their cameras upon completion of the course.
Instruction included an introduction to a range of photography genres, training strategies in the use of digital cameras, and practice with the Adobe Photoshop Elements imaging software program that allowed editing and production of exhibit-quality prints.
Weekly homework was assigned and students were encouraged to maintain a personal journal for the purpose of creating photograph captions and artistic statements for exhibitions.
Over each five-month course, students progressed from beginner to intermediate, and, finally, to an advanced level. Upon completion, each student produced up to 10 finished photographs to be framed and showcased in a program-specific exhibition at Rancho attended by their peers, hospital staff, and members of the community.
Special Activities. As the program grew, special activities were created to support the insights and talents of the attending students.
Field trips. To provide more opportunities to take photographs in community settings, the program included field trips to such locations as a Japanese garden, Venice Beach, Chinatown, the Getty Museum, Santee Alley, and the downtown Los Angeles Arts District. During some outings, the students shared meals in restaurants, which helped foster their growing camaraderie.
Guest speakers. Each semester, several professional photographers from the region gave pro-bono presentations offering various perspectives and genres of photography to broaden students’ exposure to artistic approaches and interpretations. Speakers included:
- John Free: World-renowned street photographer and social documentarian who has taught classes at USC, UCLA, and the L.A. County Museum of Art. See his involvement at this YouTube link.
- Rafael Gardenas: Self-taught photographer who captures moments of vulnerability in portraits, landscapes, and architecture, allowing him to explore his relationship with the streets of East Los Angeles. Gardenas has been featured in the Los Angeles Times and has released a book of his photography.
- Deb Halberstadt: Former manager of NBC’s Media Services-Photography for Corporate Communications. She has worked for the Associated Press as a picture editor and photographer.
Wheel of Mayhem Game. To help promote student engagement and participation, the project coordinators created an innovative game. Whenever students completed their photography homework, presented a journal entry, offered a thoughtful critique of another student’s work, mentored another student to develop their skills, or were awarded the best photo of the week, a ticket with their name was deposited in a jar. The more activities that were completed, the more tickets were placed in the jar for a chance to win a camera at the end of the course. Additionally, at the beginning of each class, the instructor would pull a ticket from the jar and the chosen student would spin a roulette wheel. Depending on where the arrow landed, the student could win or lose tickets (Addendums 1-2.) This game proved quite motivational and popular with students.
Evolution of the Program
Based on the experiences and feedback from the first year of the pilot, the following changes were made:
Class Frequency. The original intention was to hold a four-hour class once a week. However, because of space limitations, the class was instead divided into two three-hour sessions, which had the added benefit of greater one-on-one time with the instructor.
Transportation. Attrition due to limited transportation options for people with physical disabilities proved to be an important factor in the first year of the project (Table 1.) By the third program year, the following services were included in the budget:
- A chartered bus for field trips
- Travel stipends for students who were able to provide their own transportation
- Special-purpose, free transportation for those students who could not provide their own transportation
Student Requests for Additional Content. After the first year, several graduates expressed interest in taking additional courses in self-leadership, peer mentorship, and career development so that they might pursue a career in photography. These components were incorporated into later program years via guest speakers and the introduction of teaching assistants.
Teaching Assistants. Two photography program graduates joined the 2016 and 2017 programs as paid teaching assistants. They added several important benefits to the class:
- Providing a level of education, support, mentorship, and skilled resources that only fellow peers can offer
- Creating a video with the students to document their experiences
- Using the program’s social media sites to raise awareness about the RRI photography program, network, and collaborate with community resources
- Inspiring both beginner and advanced students to further explore photography and other forms of art as therapeutic recreation and possible employment
- Serving as guest speakers after having gone on themselves to pursue opportunities in photography, video, and art
From the authors’ perspective, the introduction of the teaching assistants considerably improved the learning experience and confidence reported by students of both years. Indeed, recent research shows that receiving peer support promotes participation and life satisfaction for adults with SCI.12
Outcomes
Creative Productions
Photography Exhibitions. At the end of each semester, selected photographs were displayed for sale at a public exhibition at Rancho. The students’ photographs were frequently poignant and thought-provoking. Craftsmanship was also apparent with aesthetic richness and the technical control of light and exposure.
Figure 3: Big City Dreamer (Photograph by Jerry O’Brien.)

Student Recognition. Positive community response resulted in many students being recognized for their work. At the 2014 exhibition, $1,000 worth of photographs were sold; in 2016, $1500; and in 2017, $540 in a single exhibition. All the proceeds went directly to the students, offering realistic validation of a possible new career goal. The course evaluations showed that the students appreciated having the opportunity to display their work in a photography exhibition.
In 2015, several graduates also exhibited photographs at the Annual Art Show at the Aquarium of the Pacific in Long Beach, California.
Exhibition Catalogues and Photography Books. Exhibition catalogues and high-quality hardcover photography books were produced for both the 2014 and 2016 program years. With the inclusion of biographical statements, these served as a personal portfolio for students.
Web Gallery. The project coordinator updated and maintained the RRI web gallery (https://www.ranchopix.com)for one year following each pilot program. The gallery featured biographies of the students and an online portfolio of their work.
Qualitative Themes
Upon graduation, students were asked to give feedback on the program. In addition, students in the 2017 program took part in a video interview. Their responses were consistent with the areas of positive transformation identified in the paper by Chun and Lee1 and are categorized below:
Theme #1: Opportunities to discover abilities and hidden potential
“One thing that I’ve learned about myself through this course is that I have a natural eye for photography. The first really good picture I got was a week into the class. It’s actually the picture that’s on the cover of our class photography book.” –Daniel Alvarez.
Figure 4: Stairway to Heaven (Photo by Hobal Grajeda.)
“I love that photography is something I can do by myself. It gives me a sense of accomplishment and improves my self-esteem. Photography has changed the way I see the world and through my photographs, I show others how I experience the world.” –Hobal Grajeda

Theme #2: Making sense of traumatic experiences and finding meaning in everyday life
“The class has encouraged me to see what life is really about. Instead of staying home and feeling sorry for myself, I go out with my camera and shoot interesting things. I’m meeting more people, and I’m experiencing things I wouldn’t have experienced before. I’m enjoying life now. I feel much more confident and very independent.” –Michael Lopez
“The photography course has taken my disability away because I’ve been out more. It just kind of opened my eyes to a whole new world of things to do.” —Daniel Alvarez
Theme #3: Generating positive emotions
“I have gotten used to being in chronic back pain daily but getting out to do photography really helps me push myself to do more, and my clinical depression gets better when I’m involved in the program.” –Jerry O’Brien
“I feel more independent since taking this course just because it’s taken me out of my house more and I’m doing a lot more. And it’s really helped me a lot. I find myself in the street a lot more during the week that otherwise I would spend at home.” –Daniel Alvarez
Other positive emotions mentioned by students included increased relaxation, pride and a sense of accomplishment, more confidence, and feeling empowered through learning a new skill.
Theme #4: Building companionship and meaningful relationships
“The encouragement that I’ve gotten from the instructor, Michael, and from my classmates has helped to open my eyes to a whole new world of possibilities.” –Daniel Alvarez
The project coordinators and staff observed strong friendships forming among individuals who might never have met under other circumstances. Students supported each other throughout the course, offering constructive critiques and assistance. Several even created their own assignments wherein they scheduled days to meet and photograph each other’s hometown. These emotional connections continued even after completion of the course. Graduates regularly shared information on new techniques and better photographic practices. Some showed their work in other venues and these events were well-attended by their classmates. The relationships these students established were not just defined by photography but expended past the classroom environment and into the realm of true, long-term friendships.
Although the effectiveness of a program is usually considered in terms of population groups, aggregate measures cannot fully convey the impact on individual participants. To help illustrate the latter, the authors have included Melissa Allensworth’s story. Her words paint a compelling picture of the photography pilot from a personal perspective.
Melissa’s Story
Melissa Allensworth was only 27 years old when she suffered a complete T4 spinal cord injury after a rollover car accident in 2008. Despite the new challenges she faced, Melissa was determined to continue living her life to the fullest. “I made it a goal early on that I wouldn’t let my injury hold me back from experiencing fun and adventure,” she says. “Once I made that decision, doors started opening. I just try to take advantage of every opportunity that’s out there.”
For Melissa, those words are not just sentiment but a way of life. Since her accident, Melissa has traveled internationally, and road-tripped across the United States. She paddleboards, handcycles, scuba dives, and takes part in the biannual wheelchair sports festival. One of her proudest accomplishments is the pilot’s license she earned through Able Flight, an intense seven-week program that teaches individuals with disabilities how to fly airplanes. Melissa also volunteers as an outreach representative for the Triumph Foundation, a non-profit organization that provides hope and resources to individuals with SCI. “It’s been really fulfilling to be connected with this program, to give back and let people know that’s there’s still life after disability,” she says.
But it is Melissa’s creativity that has, like a siren’s song, irresistibly beckoned to her throughout the years. Early on, she had planned a career in film making and graduated from the Art Institute of Los Angeles with a degree in video production. Melissa later realized, however, that she had her own creative vision and was not happy making other people’s movies. After her injury, she instead began painting and was awarded an artist residency at the Vermont Studio Center. Melissa subsequently became a professional artist, exhibiting her work in gallery showings and on her website.
Despite these accomplishments, there was one door Melissa believed to be permanently closed. “After I was injured, I thought, ‘Oh my gosh, I can’t take photos again because I’m sitting in a wheelchair. I only have this one angle now. I can’t see things,’ ” she says. Melissa just assumed her photography days were behind her.
Once Melissa enrolled in the photography pilot program, however, she realized her beliefs had been holding her back from her true potential. “My view of my injury and myself was limiting,” she says. “The class helped expand that. It completely changed my perspective and point of view. You’re just limited by your mind. I saw I could do more than what I thought I could.”
After gaining confidence through seeing the public appreciate and buy her creations, Melissa has now added photography to her artistic repertoire. “It’s all about how an image makes me feel. I take a photo of the feeling I’m trying to convey,” Melissa explains. “I do a lot of work in black and white because I think it adds emotion. Color can be distracting.”
Because the spinal cord injury community is small, she frequently sees previous classmates at events, gatherings, and on social media. Melissa has remained friends with many of them and knows they have also continued to take photographs, some professionally.
Figure 5: 25 Cent View (Photography by Melissa Allensworth.)

When asked about the class’s long-term impact, Melissa says, “It was definitely life-changing. I thought I’d never pick up a camera again. Now I’m exhibiting photographs and making works of art.”
Discussion
A fundamental goal of both the proof-of-concept and pilot projects was to provide a supportive educational environment so students could develop the necessary technical and artistic skills for creative self-expression. In the article entitled “Photography and Art Therapy: An Easy Partnership,” the author states that adults with SCI “may find meaning and cohesion in their life stories through individual artmaking with photographs.”13 And according to class instructor Michael Ziegler:
“Photography is an ideal tool to engage and inspire people who are struggling with their lives. Photography combines instant, tangible gratification with the potential to rework an image to perfection and then to share with friends and strangers to get important feedback, to provide reaction and emotion…by opening students’ minds to the possibility of the entire photographic process—technical skills, visualization, anticipation, artistic execution both in-camera and with the computer—we can change the focus of a troubled existence, one that might be only going through the motions of life. Students may see what they thought was an ordinary world in an entirely new way and discover the thrill of being able to capture that new vision and put it on paper or on a website to share with others.”
Although further studies would be needed to gauge the true long-term impact, it appears from the aforementioned outcomes, feedback from the students, and the program coordinators’ observations, that the pilot program met its goal. Through their artistic achievements, students gained confidence in their abilities. They began to see the world through new eyes. Many became friends, providing emotional and practical support for each other. They learned skills that could assist in future employment: Two graduates are now employed at Rancho and at least four have pursued photography professionally. This new perspective had a profound experience on the students captured in the following quotes from two of them:
“In five years from now, after taking this photography course, I see myself being an artist. Maybe doing photo shoots, maybe even having my own photo place. You know, taking pictures of people, doing weddings because there’s a lot to do with photography. And possibly even teaching others. I love to teach, especially children. I love working with children and teaching them things.” –Michael Lopez
“I am actually into video and my view through a camera has helped a lot. To have a good eye for locations, just how to place people in the frame can help me out a lot. One of the goals I have is making a documentary about living with spinal cord injury and its effect on people.” – Daniel Alvarez
For underserved populations, programs such as the photography pilot may offer opportunities and benefits otherwise not readily available to them. Photography may also give them a voice, a way to speak their truth to a society that only becomes stronger when all its members—especially those who have been historically underrepresented—are heard. Art can serve as a powerful medium to explore different cultures and life experiences while also uniting people in their shared humanity.
Figure 6: Unseen (Photograph by Jonathan Alvarenga.)

Conclusion
The outcomes of this pilot educational program suggest that recreational photography can be a powerful modality in the psychosocial wellbeing and ongoing rehabilitation of adults with SCI. In addition to the obvious social aspects, the authors observed an improvement of mood, development of artistic and technical skills, increased confidence, and excitement for the artistic process. Albert Bartee III, a student of the pilot program, summarizes this well in the following quote:
“It’s helping me to develop more patience, maintain my strength, as well as improve my communication skills, and even my people skills. During photography, you come across obstacles. When I’m shooting, I often ask myself, ‘What if?’ and thinking about difficulties as things that can be beautiful instead of obstacles has made me look at my life differently. That is something for which I am very grateful.” —Albert Bartee III
In many ways, the pilot helped bring together the students and the Rancho professional community. Students’ photographs can be found throughout the campus; the photography exhibitions have been well attended by staff, and graduates are frequently approached to serve as photographers for various Rancho-sponsored activities.
During the American Hospital Association’s 2011 roundtable on Workforce Roles in a Redesigned Primary Care Model, it was recommended that hospitals serve as catalysts for linking and integrating various components of health and wellness together for patients in a sustainable infrastructure.14 To that end, RRI is actively exploring new avenues to ensure the long-term success of the photography program. Plans for the next phase include online lectures by professional photographers, community-based Meetups, and biannual photography competitions. Any adult with disability in the Rancho community will be welcome to participate. The project coordinators also intend to seek out collaboration with other institutions to create a community of like-minded artists and rehabilitation providers.
The authors hope that the disseminated results of this pilot will lead to improvements in the approach of rehabilitation care and educational programs for adults with SCI. It could serve as a model for the incorporation of visual arts production during neurological rehabilitation in order to support meaningful engagement in recreational activities. The proliferation of similar programs could only improve the well-being and independent living of these individuals. Furthermore, photography as therapeutic recreation and art therapy could be offered to other populations of people living with chronic disabilities with possibly similar benefits.
Figure 7: The Dog (Photograph by Ramon Cervantes.)

The authors would like to extend special recognition to Charles A. Stewart, MD, for his encouragement, support, and steadfast advocacy of this program. The authors also thank Spencer Toledo, Sandra Avina, Sheetal Desai, MD, Linda Sutherland, and Stephanie Bughi for their invaluable contributions, as well as Ginte Jasulaitis, MD, and Stephen Arthur, MFA, MSc, for providing the writing and editing of the article.[/vc_column_text][vc_column_text]
Funding
This project was supported in part by Grant Nos. 280512 and 361725 from the Craig H. Neilsen Foundation and Grant No. 90PR3002-02-01 from the Christopher and Dana Reeve Foundation.
1. Chun S, Lee Y. The role of leisure in the experience of posttraumatic growth for people with spinal cord injury. J Leisure Res. 2010;42(3):393-415. https://www.nrpa.org/globalassets/journals/jlr/2010/volume-42/jlr-volume-42-number-3-pp-393-415.pdf
2. Iwasaki Y. Leisure and meaning-making: implications for rehabilitation to encourage persons with disabilities. J Voc Rehabil. 2017;46:225-232.
3. McVeigh DA, Hitzig SL, Craven BC. Influence of sport participation on community integration and quality of life: a comparison between sport participants and non-sport participants with spinal cord injury. J Spinal Cord Med. 2009;32(2):115-124. https://www.ncbi.nlm.nih.gov/pubmed/19569458
4. Kleiber DA, Brock SC, Lee Y, Dattillo J, Caldwell L. The relevance of leisure in an illness experience: realities of spinal cord injury. J Leisure Res. 1995;27(3):283-299. https://www.calvin.edu/~y133/documents/Relevanceofleisureinanillnessexp95.pdf
5. Boschen KA, Tonack M, Gargaro J. Long-term adjustment and community reintegration following spinal cord injury. Int J Rehabil Res. 2003;26(3):157-164. https://www.ncbi.nlm.nih.gov/pubmed/14501566
6. Pentland W, Harvey AS, Smith T, Walker J. The impact of spinal cord injury on men’s time use. Spinal Cord. 1993;37(11):786-792. https://www.ncbi.nlm.nih.gov/pubmed/10578250
7. Tasiemski T, Kennedy P, Gardner BP, Taylor N. The association of sports and physical recreation with life satisfaction in a community sample of people with spinal cord injuries. Neurorehabil. 2005;20(4):253-265. https://www.ncbi.nlm.nih.gov/pubmed/16403994
8. Benony H, Daloz I, Bungener C, Chahraoui K, Frenay C, Auvin J. Emotional factors and subsequent quality of life in subjects with spinal cord injury. Am J Phys Med Rehabil. 2002;81(6):437-445. https://www.ncbi.nlm.nih.gov/pubmed/12023601
9. Bolwerk A, Mack-Andrick J, Lang FR, Dorfler A, Maihofner C. How art changes your brain: differential effects of visual art production and cognitive art evaluation on functional brain connectivity. PLoS One. 2014;9(7):e101035. https://www.ncbi.nlm.nih.gov/pubmed/24983951
10. LaVela SL, Balbale S, Hill JN. Experience and utility of using the participatory research method, photovoice, in individuals with spinal cord injury. Top Spinal Cord Inj Rehabil. 2018;24(4):295-305. https://www.ncbi.nlm.nih.gov/pubmed/30459492
11. A Class Act: Photographs From the Students of Rancho’s Research Institute’s Inaugural Class (February-June 2014). Downey, CA: Rancho Research Institute; 2014. (Exhibition catalogue.)
12. Sweet SN, Noreau I, Leblond J, Martin Ginis KA. Peer support need fulfillment among adults with spinal cord injury: relationship with participation, life satisfaction, and individual characteristics. Disabil Rehabil. 2016;38(6):558-565. https://www.ncbi.nlm.nih.gov/pubmed/26017541
13. Kopytin A. Photography and art therapy: an easy partnership. Inscape. 2004;9(2): 49-58.
14. Aquarium of the Pacific’s 12th Annual Festival of Human Abilities Features Performances and Free Art Classes for Everyone [press release]. Long Beach, CA: Aquarium of the Pacific; 2015.
15. Workforce Roles in a Redesigned Primary Care Model. American Hospital Association; 2011. http://www.aone.org./resources/primary-care-workforce-needs.pdf
Addendum 1: Roulette Wheel in Wheel of Mayhem Game
 [/vc_column_text][vc_column_text]Addendum 2: Explanation for Roulette Wheel in Wheel of Mayhem Game
[/vc_column_text][vc_column_text]Addendum 2: Explanation for Roulette Wheel in Wheel of Mayhem Game
If you land on…
| …here’s what happens. |
| 2 – for – 1 | For every ticket you earn during this class, you get an additional ticket. Two for the price of one! |
| Biggest Loser | Lose 3 tickets. |
The Replacements | Take out 3 of someone else’s tickets (your choice!) and replace them with 3 of your own. |
You be the judge! | You’re the judge of today’s photo contest! You may award 2 tickets for first place, 1 ticket for second place. You are allowed to choose your own photo! |
Ride-or-Die Homies | Choose a friend. We’ll hold two cards behind our backs, one in each hand – an angel card and a devil card. You pick a hand. If you pick the angel card, you and your friend each win 2 tickets! If you pick the devil card, you both lose 2 tickets. |
Evil Sandra | Sandra chooses what happens here. She’ll either choose one of the existing scenarios or come up with one on the fly. You’d better be nice to Sandra lest she smite you a mighty blow! |
Dice of Destiny | Roll each of two colored dice. The darker die is the bad die, the lighter die is the good die. Whichever die has a higher number, you gain or lose that many tickets. |
| Sophie’s Choice | You have two choices: You can either a) take 3 additional tickets for yourself, OR b) remove 3 of someone else’s tickets. |
Small Jar | The small jar contains everyone’s name twice. Each name in the jar has either a thumbs up or thumbs down on it. We’ll pick one name out of the small jar, and depending on which ticket is picked, that person will either gain or lose 3 tickets. |
Wild Card | You get to pick any of the scenarios on the Wheel of Mayhem, OR you can choose to put your ticket back in the jar, OR you can try your luck at one of the mystery boxes. |



In June 2017, I was a 63-year-old runner, long-distance open-water swimmer, hiker, hobby photographer, and middle-school science journal editor. I had been weight-training for 15 years. Had I been born decades later, I would have been diagnosed as hyperactive. I often thought that a hyperactive child is frustrating for adults, but being a hyperactive adult is great because you have abundant energy.
In July 2017, I experienced an ischemic stroke in my right cerebral hemisphere. I was affected on my left side following my stroke and I am left-dominant. At the time of my stroke, I did not understand the severity of my injury. I was optimistic because my body had never let me down. I was sure I would be back to my active self within a few months, even though a physician friend told me I would spend a year in recovery, if not longer. I began reading about stroke recovery while in inpatient rehab. Slowly, I began to understand that my condition was worse than I thought, and I had a long road to travel. I never doubted, however, that I would recover. I just needed to figure out how to do it.
Painting as a Healing Art
I contemplated painting as a hobby just before the first anniversary of my stroke, since so many of my favorite more rigorous activities were restricted by the stroke’s effects. I had painted years before, although photography had been my more recent medium of choice. I probably would have focused on photography as a hobby, except that my mobility was insufficient to walk where I like to take photos and my left hand and wrist would not move adequately to make photography a practical hobby at that point in my ongoing recovery.
When I told my Emory neurologist, Dr. Samir Belagaje of my plan to begin painting, he advised, “Paint with your left hand!” I realized the wisdom in this suggestion. Painting with my affected hand would provide needed fine motor movement for rehabilitation purposes. I had rejected other standard hand therapies, such as putting lids on jars, and even repetitive computer-based therapy games. I found them boring. I knew I did not need to spend more time in front of a screen. I wanted to be creative.
All the images in this essay were created following my stroke. Using my left hand to draw and paint has facilitated my hand’s and wrist’s fine movement, although recovery remains slow, even 18 months past my first painting (2.5 years post-stroke). Each image in this essay is accompanied by a short narrative that explains its significance as a physical therapy. At the beginning, I approached each project with its specific movement requirements in mind, exercising different arm, hand, and wrist muscles as required by the medium.
This narrative, therefore, describes an exploration of my brain’s neuroplasticity, my struggle for fine motor control in my affected hand and wrist, and my journey creating art, no matter the result.
My Journey
 July 2018: Boat in Loch Harray, Orkney Islands, Scotland, tempera
July 2018: Boat in Loch Harray, Orkney Islands, Scotland, tempera
My husband Ken and I travel to Scotland every other year. In 2017, we visited Scotland’s Orkney Islands. This boat had been pulled onto Orkney’s Loch Harray shore, just a few hundred feet from our hotel. I have an affection for row boats, having spent many hours in my teen years rowing one like this. I took a photograph of the boat and painted from the photograph. The photograph was taken about 2 months before my stroke in 2017.
This was my first painting after my stroke, and I finished it just one day shy of my first stroke anniversary. I decided to use tempera paint because it is inexpensive and easy to use. I had no idea what to expect. My main goal was improved movement, not great art. Although the painting is rough, I was surprised that I had any hand control at all.
 September 2018: St. Clements Church, Isle of Harris, Scotland, tempera
September 2018: St. Clements Church, Isle of Harris, Scotland, tempera
This painting was done from a photograph I took in 2015 on the southern tip of the Isle of Harris, Scotland. This is St. Clement’s Church, built in the late 1400s or early 1500s. Ken and I have visited this church at least four times, and its exterior architecture and interior sanctity have always captured my affection and provided inspiration.
With this painting, I discovered that I could be more successful at painting if I dabbed paint on the paper. This was an important discovery because my wrist would not bend, and brush strokes, therefore, were challenging.
 November 2018: Moonlight Through Church Window, tempera
November 2018: Moonlight Through Church Window, tempera
This window is in a corner of our bedroom. Early one August morning in 2018, I woke up to see light from the setting full moon flowing through the glass. I got up, took a photograph, and painted this painting from that photograph.
This was further experimentation with the dabbing technique first tried in September. Dabbing gave me a way to paint without using my wrist, which still would not extend. I also found it hard to hold the brush. Dabbing gave me ample opportunity to rest between “dabs” as needed, but I dropped the brush many times and had to cover up unwanted paint blobs.
 October 2018: Tallassee Oak, charcoal and pastel
October 2018: Tallassee Oak, charcoal and pastel
This majestic white oak is growing beside my house. It is hundreds of years old, and it takes four people holding hands to surround the trunk.
Dr. Rich Panico, my meditation teacher and an artist, recommended that I try charcoal on large paper to give my entire arm an opportunity to practice control. I decided to add pastel chalk because I like to use color. I found it difficult to control charcoal and pastels. I dropped (and broke) many pieces of chalk while drawing this tree. The trunk is lighter at the top because the evening sun was illuminating the upper part of the tree. All I could do was scratch and scribble; drawing small shapes was out of the question.
 January 2019: Southern Utah, colored pencil
January 2019: Southern Utah, colored pencil
This drawing was from a photograph I took in 2014 while Ken and I were traveling in Utah.
I felt that my wrist needed an opportunity to practice extension, so I decided to try colored pencils. I had never used colored pencils before. In this effort, I found it difficult to press hard on the paper, extend my wrist to complete the pencil lines, hold the pencil, and maintain control. This drawing exhausted me. You can imagine how pencil lines require wrist flexion and extension, and perhaps understand the challenge I faced. This drawing experience, in spite of its difficulty, was much more rewarding to me than handling jar lids or folding clothes.

 January 2019: South Harris Beach, Scotland, colored pencil and tempera
January 2019: South Harris Beach, Scotland, colored pencil and tempera
The Outer Hebridean Isle of Harris is known for its tweed and its white sand beaches. These two drawings were done from the same photograph, most likely taken in 2013.
Have you ever tried things that just did not work? Emboldened by my colored-pencil experience, I tried another pencil drawing and became so frustrated that I allowed my right hand to help. The result was sub-par. I tried the same scene with tempera, with an equally undesirable result. At least my left hand had more practice. I love water landscapes, but this experience taught me how hard water is to capture in drawings and paintings.
 February 2019: Tuckasegee River, Nikon 7200 DSLR
February 2019: Tuckasegee River, Nikon 7200 DSLR
The Tuckasegee River is in the mountains of Western North Carolina. It is one of my favorite rivers to photograph, since the water is clear and therefore reflects colors and light in a wide variety of delightful ways.
Prior to my stroke, one of my favorite hobbies was photography. I particularly like to photograph the surface of natural waters. My stroke inhibited my using my Nikon DSLR in three ways: 1) I could not turn the zoom lens with my left wrist; 2) the camera was too heavy to easily use with one hand; 3) I could not walk or move into proper position for my desired photo, which was often in hard-to-reach natural settings. This photograph marks the first time I was able to move into a position that enabled me to get the photograph I wanted. The riverbank was just a small downhill (and grassy at that!), but it was an important accomplishment for me.

 March 2019: Brain Stroke/Brush Stroke, tempera
March 2019: Brain Stroke/Brush Stroke, tempera
I volunteered for a clinical trial at Emory University in early 2019. I discussed my painting projects with Dr. Trisha Kesar, the principal investigator. Dr. Kesar showed me a painting she had done of a human brain. It was lovely and I was inspired. While preparing for a presentation about my stroke recovery journey, I decided to quickly paint my own brain with its ischemic stroke and its subsequent recovery process to use on the cover slide.
Immediately after finishing the paintings, I felt an almost imperceptible improvement in my overall condition. Describing such a small improvement is difficult. Did I just imagine it? The effect was not tangible. The best way to describe it was as knowledge of a small shift toward improvement in my brain and body. That experience of improvement inspired me to try some additional “self-portraits,” with a different twist.
 April 2019: Brain to Deltoid Connection, charcoal and pastel
April 2019: Brain to Deltoid Connection, charcoal and pastel
After reflecting on what I felt was a small shift resulting from my brain paintings (Brain Stroke/Brush Stroke), I wondered if drawing the brain-muscle connection would have any effect on my recovery. I knew that visualization was recommended as a stroke-recovery therapy (so of course I tried it). Visualization, as I understood it, involved imagining a desired movement in detail. I, for example, imagined in detail swimming or running. This imagining experience was entirely internal and focused on movement. Enlisting my eyes, I reasoned, would enhance the chances of facilitating the desired brain-muscle communication, literally showing my brain what I wanted it to do. I know that people often learn by watching and/or by doing. I thought that I would combine these known learning techniques for stroke recovery, taking visualization a step further and closer to the genesis of movement.
This drawing was my first attempt to visually show my brain what I wanted it to do. In this drawing, I wanted to improve my brain-to-deltoid nerve connection. Prior to completing this drawing, my deltoid was tested using electromyography (EMG) and found to lack innervation. The doctor who did the EMG told me that I would never have use of my deltoid again. I could lift my left arm only about 10 degrees to the side. I believe the drawing helped to reestablish or support the nerve reconnection. Within a few days of completing this drawing, I was able to lift my arm to about 45 degrees using the deltoid. Note that the connection I’ve drawn is between the right brain hemisphere and my left deltoid. After completing a few more of these brain-to-muscle drawings, I named this technique autophysioartistry, or APA.
 April 2019: Brain to Hand Connection, charcoal and pastel
April 2019: Brain to Hand Connection, charcoal and pastel
Following the deltoid experience, I drew three more APA drawings using a pencil. I “knew” that my mobility was improving as I completed more APA drawings. The deltoid example was dramatic and measurable, but subsequent brain-to-muscle connections were not as easily measured.
After completing the trio of APA pencil drawings, I determined that pencil lines were too timid. I tried another charcoal and pastel drawing. This drawing feels like it has power to convey to my brain what I want it to do.
 May 2019: Woodland Ransome Wildflowers, Lake District, England, Nikon DSLR 7200
May 2019: Woodland Ransome Wildflowers, Lake District, England, Nikon DSLR 7200
In May and June 2019, Ken and I traveled to the UK. On the way to Scotland, we traveled through England’s Lake District. As we drove north, I noticed a blanket of white on the forest floor.
Getting this photograph required my walking through thick waist-high vegetation while holding my Nikon camera above the vegetation. Another first in my recovery journey! I would have not tried the short but weedy trek if it had not been for the lovely landscape and my desire to photograph it. Taking this photograph made me feel like I was making progress toward my pre-stroke self.
 June 2019: Village Bay, Hirta, St. Kilda, Scotland, Nikon DSLR 7200
June 2019: Village Bay, Hirta, St. Kilda, Scotland, Nikon DSLR 7200
During our Scottish travels, Ken and I visited St. Kilda archipelago 50 miles off the Scottish west coast. St. Kilda is only accessible to visitors who endure a 3-hour boat trip across the often-turbulent north Atlantic Ocean. Ours was a small boat that accommodated 12 passengers with an open area in the back of the boat. As we left St. Kilda, I saw these lovely colors and wanted to capture them, even though the boat was accelerating and was somewhat unsteady.
I needed to use both hands to get the shot from the back of the boat. Getting this photograph required balance and quickness.
 July 2019: Kingfisher Creek, Olympus Tough (camera)
July 2019: Kingfisher Creek, Olympus Tough (camera)
Kingfisher Creek marks our property line in Georgia. The creek is located down a series of old cotton terraces through what is now mature forest. The way is relatively steep with no trail. The walk is pleasant, but it is a difficult task for a person relearning to walk. I love this creek and have felt solace for more than 35 years sitting along its banks.
On this morning, I walked alone to the creek for peace, exercise, practice, and to take photographs. Getting to the rocks at the water’s edge required my maneuvering down a steep but short bank. I suppose I risked falling but I used my walking stick for support. This experience gave me confidence and boosted my feeling of independence.
 July 2019: Purple Mountains, watercolor pencil
July 2019: Purple Mountains, watercolor pencil
In early spring 2019, a salesperson at my local artist-supply store suggested I try watercolor as a part of my art physical therapy. I had never used watercolor and was reluctant to try it, given my lack of control and unfamiliarity with how to paint with watercolor. Then coincidentally, prior to joining us during our UK vacation in June 2019, friends had visited a pencil museum and were given four watercolor pencils as a parting memento from the museum. They gave their pencils to me. I decided to give the pencils a try, and painted this scene using the four colors. The salesperson was correct about watercolor’s physical therapy benefits—or at least watercolor pencils’ benefits.
The initial pencil strokes required wrist movement like that with colored pencils, and the followup brush strokes required a more fluid, whole-hand motion. Only having four colors required me to vary the pressure of the pencil stroke to create color variations in the wheat. I found that I was only marginally successful using watercolor pencils. They are a medium that might require expert instruction.
 July 2019: Swim, pencil, charcoal, and pastel
July 2019: Swim, pencil, charcoal, and pastel
I love to swim. Before my stroke, I swam three long-distance, open-water swims every year. I have an endless pool at home, so I had logged many hours swimming. Swimming requires strong deltoid muscles, strong shoulders, the ability to straighten your arm and hand, and an even kick.
This APA drawing was meant to stimulate and support the right motor cortex-to-deltoid and right motor cortex-to-hand connections. It’s difficult to say whether it helped me with swimming, given my need to simultaneously strengthen my recently innervated deltoid. To complicate my recovery, in November 2018 I had torn my left rotator cuff trying too hard to swim the crawl (and doing Downward Dog yoga poses) before my body was ready. Waiting until my body is ready to move in more advanced ways was a bitter but important lesson for me. However, every day I am closer to swimming the crawl properly and I believe this drawing reminds my brain that swimming is a goal.
 July 2019: Run, pencil, charcoal, and pastel
July 2019: Run, pencil, charcoal, and pastel
I love to run. Pre-stroke, I ran 3 to 4 times every week. I have completed 6 marathons. The day after my stroke, the Hospitalist told me I would never jog or run again. Why would a medical authority figure limit a patient’s recovery with such a negative pronouncement, especially so early after the stroke? Recall that I had faith in my body to recover and did not understand the severity of my injury. That dire prediction was all I needed to hear to determine that I would one day jog and run again.
I have begun to slowly jog; not too far or for too long, but that will come. Running requires a functioning connection between the motor cortex and the anterior tibialis (purple line) and soleus (orange line) leg muscles. The anterior tibialis is used in the heel-strike phase, and the soleus is used to push off with the toes. In this APA drawing, I added the deltoid connection (red line) for fun.
 July 2019: Magnolia, tempera and colored pencil
July 2019: Magnolia, tempera and colored pencil
Many years ago, I took a photograph of a magnolia bloom in our yard. I always loved that photograph, so I thought I would try another dabbing project. I was not as pleased with the result as I had hoped.
As I dabbed, I kept thinking that this painting would look better with brush strokes. I thought I should have tried using brush strokes since my wrist was extending much better. Additionally, dabbing is a time-consuming technique. I was impatient to continue trying new ways to move my hand and wrist.
 August 2019: Smile, pencil, charcoal, and pastel
August 2019: Smile, pencil, charcoal, and pastel
I consider mouth drop a barometer of my progress. The zygomaticus major muscle enables us to smile. I felt an improvement in my smile after drawing this brain-to-zygomaticus-muscle connection. I could pull my lip up farther than I could previously, and Ken confirmed the improvement. In November 2019, my primary care physician commented that I had no face drop at all! That was not an accurate assessment on her part, but I am getting closer. I feel that when my smile is complete, my full recovery will not be far behind. If you can smile, do it often!
In September and October 2019, I was given the opportunity to hang a show of my artwork in a local restaurant. Having this show gave me a deadline that urged me to continue painting throughout the summer. I was overwhelmed by the support I was shown at the opening reception and throughout the show. I included a short explanation of each image, hoping to educate others about the effects of stroke and the possibility of recovery.
 October 2019: Guzei, pastel
October 2019: Guzei, pastel
Ken and I visited Butchart Gardens, Victoria, British Columbia, in September 2019. I fell in love with the Japanese Garden. Japanese gardens are meant to connect people with nature and to encourage reflection and meditation. One of my other therapies is a daily meditation practice; I enjoyed the Japanese Garden immensely. Since my wrist was extending better and I had found some success with my APA pastel drawings, I thought I would try doing another landscape drawing with pastels. I did this drawing from a photograph I took in the Japanese Garden. A guzei is a red Japanese bridge, and it has spiritual significance as a symbol of transformation.
I found that landscape drawing with pastel, which I had not tried since I drew the Tallassee Oak a year earlier, was frustrating because I still could not draw and fill in small shapes. I felt like I could only move forth and back with the pastel chalk, scratching and scribbling. Round and curvy shapes were still elusive. A comparison of this drawing with the Tallassee Oak drawing will allow you to draw your own conclusions about my improvement over the 12 months between drawings.
 November 2019: Japanese Garden, pastel
November 2019: Japanese Garden, pastel
I was determined to try another pastel drawing. This time, I wanted to concentrate on small, curvy shapes. One thing I did not count on was how readily pastels smear if you rest your hand on the paper, even briefly, while drawing. I needed to rest my hand to draw the small and curvy shapes that I wanted to create.
Although I had just purchased a larger pastel set with more colors, I was also frustrated with my inability to blend colors. In contrast, with tempera I could blend the paint to create any color. I could hold the pastel chalk better than in earlier pastel drawings, but I continued to find proper holding a challenge.
 November 2019: Shoulder Connections, pastel
November 2019: Shoulder Connections, pastel
Recall that I was rehabilitating a torn rotator cuff at the same time I was strengthening my deltoid. In November 2018, an orthopedic surgeon had told me that one of my rotator-cuff tears was a “probable full surface tear” that would never heal, but that surgery was out of the question because I would need a functioning deltoid to do the post-surgery rehabilitation. A year later, I was strengthening my deltoid and gently using my rotator-cuff muscles. I cannot be sure of success, but my goals are to fully strengthen my deltoid and to avoid rotator-cuff surgery. With these goals in mind, I decided to expand my APA drawing to include rotator-cuff healing.
This APA drawing is showing my brain (and body) that I want it to enlist my heart in healing by sending blood to my rotator-cuff muscles. I also included the brain-to-deltoid nerve connection, because I figured I cannot overemphasize my deltoid’s innervation. I would need another MRI to know if my rotator cuff is healing; however, I continue to gently use these muscles during my thrice-weekly weight-training workouts.
 November 2019: Relaxing the Muscles, pastel
November 2019: Relaxing the Muscles, pastel
Despite my continual improvement, I knew that one of my biggest challenges is tone (or spasticity). I needed to find a way to reduce tone in my left bicep, thumb and fingers, calf, soleus, and ankle. Other than Botox and muscle relaxers, no one had any recommendations for reducing tone. I began a self-designed program of targeted stretching and brought out my pastels for another APA drawing to reinforce the message of relaxation. I asked several friends and therapists for advice on how to draw relaxation. A friend who is an accomplished artist suggested wavy lines.
This APA drawing shows my brain that I want my muscles to relax. I was so excited about this drawing I drew myself out of proportion! One of the advantages of drawing and painting with a hand affected by stroke is that your inner art critic is no longer in charge. I did this drawing at the same time I was stretching twice daily, so it is impossible to conclude whether my improvement was a result of one, the other, or both therapies.
 December 2019: Near Machrie Moor, Isle of Arran, Scotland, tempera
December 2019: Near Machrie Moor, Isle of Arran, Scotland, tempera
I wanted to come full-circle to close this essay with another “brush-stroke” painting. Recall that when I dabbed “Magnolia” in July 2019, I thought that the magnolia would be better depicted using brush strokes. The thought of trying another brush-stroke painting stayed with me. I created “Near Machrie Moor” so that you may compare it with my first painting, “Boat in Loch Harray.” Both were done with tempera using brush strokes over just a few days. With this more recent painting you can judge for yourself whether I have made progress with my hand and wrist mobility.
As I painted “Near Machrie Moor,” I felt that I had significantly better control of the brush. Unfortunately, better brush control unleashed my inner art critic, which had previously and thankfully remained in the background. If you look closely, you can see how I painted over and over to correct mistakes. I had to force myself to declare this painting complete.
Art as a Way to Push Limits
I plan to continue my drawing, painting, and photography projects. I feel that these experiences have enriched my recovery experience and have supported my brain’s neuroplastic response. Art has been a creative and rewarding way to push my limits, and it has given me tangible evidence of progress. I am proud of my art accomplishments. Doing art reminds me to take my time and enjoy my success. It has taught me that there are no failures in my recovery, only new challenges.
In this essay, I have shared a selection of my artwork to describe how I have used art as a physical therapy for upper-limb recovery from stroke. I have done all painting and drawing independently, although I would have benefitted from expert guidance in supplies and techniques. When I began drawing and painting, I searched for information on how to heal physically through art. I found many examples of the emotional, spiritual, and social benefits of art therapy. I can attest to these benefits, as I have also experienced them through my post-stroke art projects. I did not, however, find information detailing the employment of drawing and painting to facilitate neuroplastic changes with a direct motor benefit. I feel that this literature must exist, but my searching came up empty.
Autophysioartistry as Rehabilitation Therapy
Given the imperative to foster gross and fine upper-limb movement in stroke survivors, using various art media is an inexpensive and engaging therapy available to everyone. Drawing and painting may foster neuroplasticity as well as, and more creatively than, some of the more traditional occupational and physical therapy techniques. I have only scratched the surface of possibilities. For less mobile stroke survivors, for example, perhaps collage is an option. I have experimented with photo image editing software to facilitate APA drawings by stroke survivors less comfortable with or less able to draw their bodies. I am encouraged by the opportunities made available by photo editing software and hope that others in stroke recovery will use any means available to create art—including APA—to foster their progress.
With its substantive combination of emotional, spiritual, social, and physical benefits, art should be explored, employed, and researched as a physical (and occupational) therapy for stroke survivors and others healing from upper-limb and neurologic injury. I also feel that extending visualization therapy into more concrete visualization including the brain and nervous system using APA (autophysioartistry) deserves the attention of physical and occupational therapists and researchers.
Since my stroke, I have participated in more than 30 different therapies. Many of these are standard therapies and some are novel. Based on the stroke-recovery and stroke-related research I’ve read, I created some of my own therapy techniques. This essay describes one of my self-styled therapies.

![]()
This work is licensed under a Creative Commons Attribution 4.0 International License.
The opioid epidemic has brought attention to the difficulty inherent in the medical treatment of chronic pain, a complex and multi-faceted health problem. However, chronic pain also raises questions of autonomy, an important concept in healthcare ethics. Chronic pain management programs that are multidisciplinary and utilize a biopsychosocial model with a strong emphasis on non-pharmacological therapies have become more prevalent as an alternative treatment option. These programs have a strong rehabilitative composition and espouse rehabilitative goals of empowering, guiding, and motivating patients toward involvement and responsibility in their care. The current bioethical conception of autonomy is insufficient in these programs because it presumes a static, stable self-knowledge.
Patients participating in chronic pain management programs are experiencing a dynamic, transformative process that needs a relational-creative-narrative conception of autonomy. By including expressive therapies in chronic pain management programs, patients explore and develop their self-knowledge in order to make the decisions and choices that tell their life stories. Frida Kahlo’s autobiographical art work illustrates how people living with chronic pain can understand themselves and integrate their chronic pain experiences into their lives through an expressive creative process.[/vc_column_text][vc_column_text]

Introduction
Multidisciplinary programs utilizing a biopsychosocial model with a strong emphasis on non-pharmacological therapies are today more prevalent in the treatment of chronic pain because of the opioid epidemic. While medical care has its role in multidisciplinary approaches, rehabilitation offered by physical therapy, occupational therapy, psychology, and addiction counseling is the core of these programs.1 The strong rehabilitative nature of these programs supports goals of empowering, guiding, and motivating patients toward involvement and responsibility in their care. Within these programs, respect for patient autonomy—a dominant principle in healthcare ethics—is enacted through informed consent that assumes a static, stable autonomy. Yet, patients in multidisciplinary programs are experiencing a life transition full of varying amounts of discontinuity and disorientation. Patients in chronic pain management programs must be able to exercise their autonomy in a meaningful way in order for these programs to be consistent with the moral commitments of healthcare ethics. The rehabilitative nature of chronic pain management warrants a reframing of autonomy and a reconsideration of healthcare professionals’ enactment of respect for autonomy.
This article reframes autonomy as a relational-creative-narrative concept that enables people living with chronic pain and the disability, mental health issues, and addiction that may be associated with it to untangle and interpret their lived experiences within their life stories. I explain the complexity of chronic pain and outline the multidisciplinary programs with a rehabilitation focus that are a response to the multi-faceted and complex problem of chronic pain. My claim is that autonomy conceived and enacted as a medico-legal process is insufficient for people living with chronic pain who choose to participate in chronic pain management programs. Rather, autonomy in rehabilitation requires a situated conception that considers the dynamic self-knowledge patients need in order to make the autonomous decisions and choices that integrate their lived experiences of chronic pain into their life stories.
Multidisciplinary programs support and promote such a conception of autonomy by including the use of expressive therapies, such as art therapy, music therapy, dance/movement therapy, drama therapy, and play therapy, as a treatment option. Through expressive therapies, patients have the time, space, and attention requisite to explore and develop their self-knowledge. Healthcare professionals respect their patients’ autonomy by providing a means for patients to creatively paint, write, move, enact, or play their lived experience. Consequently, patients are able to exercise their autonomy in ways that make sense of their experiences and tell a meaningful life story.2 That is, patients creatively express their autonomy as autobiography.
Frida Kahlo and Chronic Pain
The medical imagery of Frida Kahlo’s art work portraying her experiences of chronic pain has been influential in understanding patients’ experiences of chronic pain.3,4 Although engaging with the medical imagery in Kahlo’s art work may generate valuable insights for healthcare professionals, previous authors have missed an important contribution that she brings to the lives of patients themselves. People living with chronic pain and its consequences benefit from understanding their experiences within the context of their lives. Engaging in creative expression helps people explore their sense of self, make sense of their pain experiences, and meaningfully exercise their autonomy in the narrative of their lives. Kahlo’s body of artwork threads throughout this article to illustrate how she expressed a lifelong relational-creative-narrative conception of autonomy in telling her story. After all, storytelling, like pain, is as old as humanity.
Kahlo (1907–1954), a Mexican artist in the first half of the twentieth century, struggled with disability and chronic pain from her young childhood. At the age of six, she contracted polio and spent a year convalescing to recover her strength and health. As an active, vibrant child, she worked hard throughout her childhood to regain her strength—although her right leg never fully recovered. In her teenage years, Kahlo was an exceptional student and wanted to study medicine. But she also dabbled in photography and painting, because she was close to her father who was a professional photographer and amateur painter. Unfortunately, her student days ended abruptly when she was involved in a catastrophic streetcar accident at the age of 17 and spent a year recuperating and convalescing. There is no record that she participated in rehabilitation, a new healthcare field at that time; however, she received a considerable amount of medical care to address her illnesses, injuries, and chronic pain and spent lengthy parts of the last 10 years of her life recuperating and convalescing in hospitals.
Chronic Pain and Multidisciplinary Rehabilitation Programs
Chronic pain is currently entangled in the opioid epidemic—a public health crisis of opioid abuse, addiction, and overdose deaths that has become one of the biggest social problems in the United States. People living with chronic pain became involved in the opioid epidemic subsequent to the public health crisis of undertreatment of pain.
Because relief of pain and suffering is a core goal for medical practice, pain was declared the fifth vital sign in 1995 and became a key focus of medical care under the auspices of the medical model.5 Physicians were expected to treat all pain aggressively with pain medications. Aggressive pain management encompassed chronic pain as well as acute pain and pain in active cancer, palliative, and end-of-life care. Opioids, strongly and fraudulently marketed by pharmaceutical companies, became the pain medication of choice for physicians to prescribe. Due to the misinformation disseminated with little actual guidance, physicians, thinking that opioids were effective and safe in the long-term management of chronic pain, misprescribed and overprescribed opioids, with a false sense of security, for people living with chronic pain.6 The “dual public health crises of undertreated pain and opioid misuse/abuse”7 have since been problematic in the treatment of chronic pain—a complex and multi-faceted health problem.
The Complexity and Subjectivity of Chronic Pain
The medical treatment of chronic pain is complex because of its etiology, its pathophysiology, and its psychosocial effects on those living with chronic pain. First, chronic pain “arises from a complex web of heterogeneous illnesses and injuries.”17 It may occur singularly, as a group of co-morbidities, or as a series of co-morbidities. Consider the story of Jim, a healthy 43-year old, who sustains a knee injury that either does not heal well or does not recover well from surgery, which leads Jim to suffer from chronic knee pain. To make Jim’s story more complicated, he also has diabetes and is physically deconditioned as a result of working many years at a sedentary job. His comorbidities negatively affect the tissue healing in his knee leading to chronic knee pain and adding to his other health problems. Adding yet another, even more complex, layer to this medical story, Jim, with comorbidities of diabetes and deconditioning has knee surgery and develops Complex Regional Pain Syndrome, a chronic pain condition with systemic ramifications.
Next, chronic pain is defined pathophysiologically as pain lasting more than three months or as longer than what medical science understands to be the normal healing time for the affected tissue.8 However, the character of chronic pain is more complex than this definition, because it occurs at varying intensities, frequencies, and durations. As with all pain, chronic pain is a subjective report by patients that is assessed by healthcare professionals using a variety of pain scales and questionnaires. The frequency and duration of pain is also subjectively reported by patients and fluctuates with their physical activity, emotional states, and psychosocial circumstances. However, chronic pain does not necessarily follow explainable biological patterns of pathology and impairments. While all pain is held suspect because of its subjective nature, chronic pain that is disassociated from physical pathology is even more highly suspect.9 The distinct subjectivity of chronic pain makes it difficult for medical science to particularly locate the source of the pain in order to recommend, and treat with, effective medical interventions.
Last, not only does chronic pain arise from a complex web, it creates a complex web. In summarizing the psychosocial effects of chronic pain, the American Academy of Family Physicians (AAFP) states that “in addition to the physical discomfort, chronic pain causes significant work absenteeism, family disruption, and impairment of normal activities of daily living, resulting in secondary depression, social isolation, and low self-esteem among other consequences.”9 Chronic pain is a debilitating health condition experienced by people in a holistic way involving their physical, emotional, and psychosocial selves.10,11 Daniel Goldberg9 summarizes the social experience of chronic pain as silencing, stigmatizing, self-isolating, and socially alienating. The experience of chronic pain can leave people triply disabled: first by their pain, then by mental health issues of depression and anxiety, and, if opioids are prescribed inappropriately or used inappropriately, by drug addiction. The medical model grapples with adequately treating all the aspects of chronic pain.
The Multidisciplinary Treatment Approach
Recognizing the complex, multi-factorial nature of chronic pain and its medical assessment and treatment, pain researchers and government agencies have more recently emphasized treatment within a biopsychosocial model,11 with a strong emphasis on non-pharmacological therapies.12 Professionals develop multidisciplinary programs from an ethical orientation of utilizing healthcare sciences to improve the well-being of people living with chronic pain. The biopsychosocial model is enacted through multidisciplinary programs whose overarching goal is to promote patients’ active self-care and self-management.12 Typical strategies include patient-professional goal setting, patient education on the science and mechanisms of pain and chronic pain, and physical and psychological self-care. Teams of healthcare professionals from multiple disciplines work to execute the strategies of these programs.
Within the multidisciplinary teams,13 physicians provide medical evaluations and recommendations including the selection and dosing of pain medication—primarily non-opioid. If necessary, outpatient medication-assisted treatment for addiction is also provided. Nurse practitioners can also provide these medical services, and as a part of multi-interdisciplinary teams addressing chronic pain, they often regularly assess and monitor drug usage plans with patients including dosing, effectiveness, and side effects. Physical therapists provide instruction and training focused on aerobic exercise and strengthening while occupational therapists provide instruction and training focused on daily functional activities. Psychologists, counselors, and social workers provide emotional and mental health care using a variety of approaches and techniques such as cognitive behavioral therapy (CBT), stress and/or anger management, coping and problem-solving skills,13,14 and, if needed, addiction counseling. All healthcare providers integrate patient education into their care. This variety of healthcare providers represents the biopsychosocial model that provides the multidimensional care people in chronic pain need.
The structure and content of a multidisciplinary program’s protocols are developed by its healthcare professionals and based on a scientific approach to chronic pain. Through the evidence-based practice of their disciplines, various healthcare professionals delineate the specific treatment options available to patients. Programs offer inpatient and outpatient services with defined requirements of frequency and duration of attendance including a set number of weeks with specific hours each day that the patient is required to attend. Additionally, each patient follows a structured protocol of treatment interventions and activities within specific time frames, such as 30 minutes of aerobic exercise or an hour of CBT. Interventions and activities may be group-based or have both group and individual components, and are inclusive of families.11,14,15 In this manner, healthcare professionals decide what treatment options are best for and available to patients. Although care may be individualized by giving a patient the choice to ride a stationary bike or walk on a treadmill for aerobic exercise, a patient entering a multidisciplinary program agrees to follow the established protocol of the program within the limits created by the healthcare professionals through evidence-based practice.
The scientifically-established protocols of multidisciplinary approaches are rooted in the healthcare ethics principle of beneficence—which can often be, despite good intentions, paternalistic. The protocols are beneficent because healthcare professionals are acting both in accordance with, and in a manner that, contributes to the welfare of patients in their programs. At the same time, they are paternalistic because they assume healthcare science and its professionals know best how to treat chronic pain and its associated mental health conditions and addiction. Certainly, people living with chronic pain who may also be experiencing disability, depression, anxiety, or addiction are vulnerable and seek the help of healthcare professionals, hopeful that their pain can be relieved and that their lives will change in positive ways. However, paternalistic beneficence must be balanced with the moral principle of respecting patient autonomy.16
Relational Autonomy in Rehabilitation
In healthcare ethics, respect for patient autonomy is a concept that places an obligation on the healthcare professional to respect patients’ choices regarding their treatments. In multidisciplinary programs for chronic pain, once a patient is believed to have decision-making capacity, they exercise their autonomy legally through informed consent when entering a program. Through their informed consent, a patient agrees to follow the established protocol of the program. Their choices are thereby limited to the established structure, time frames, and treatment interventions offered within the protocol.
A medico-legal operation of respecting autonomy as informed consent is a “minimalist interpretation of individual and personal autonomy”17(p39) and does not adequately reflect the complexities and uncertainties of a vulnerable patient’s autonomy.17 It is also contrary to the rehabilitative goals of empowering, guiding, and motivating patients toward involvement and responsibility that are espoused by multidisciplinary programs for chronic pain.18
A Different Conception of Autonomy
Rehabilitation, as a practice of helping people recover from disabling illnesses and injuries, requires a different conception of autonomy and enactment of respect for autonomy than medicine because patients’ experiences of their autonomy are situated differently during rehabilitation. In medical contexts, the conception of autonomy is based on an either-or proposition judged by a healthcare professional about a patient’s decision-making capacity; the patient either has decision-making capacity, and thus autonomy, or they don’t. Respecting autonomy, then, is “generally no more than informed consent requirements…[which] amounts simply to a right to choose or refuse treatments on offer and the corresponding obligations of practitioners not to proceed without patients’ consent.”17(p37) Rachel Haliburton’s2 conception of autonomy that situates the person and their decision-making “within practices, narratives and tradition”2(p287) is more fitting for rehabilitation contexts. In rehabilitation, respecting autonomy involves healthcare professionals supporting the dynamic autonomy of a situated person as they adapt and adjust their value judgments and choices in the narrative of their recovery. Understanding patients’ lived experiences of chronic pain and their autonomy in rehabilitation is essential for an understanding of autonomy and of respecting autonomy in rehabilitation.
Recognizing Existential Crises
People living with chronic pain who seek multidisciplinary healthcare services are often experiencing an existential crisis.19-22 Elaine Scarry claims that pain has the “power to end all aspects of self and world.”23(p34) Not only are people in pain; their life as they have known it is lost.23 They are disoriented because every aspect of their lives—their physical and mental health, their relationships and roles, their economic welfare, and their life aspirations—is disrupted.2 They are vulnerable and seek help to learn adapting and coping strategies in order to improve their quality of life. Any disabling injury or disease disorients a person, throwing into question one’s knowledge of who they are and what values and beliefs they are enacting in their decisions and choices.2,17 For Haliburton,2 self-knowledge is needed not only to be able and free to make choices; self-knowledge encompasses knowing what values, beliefs, relationships, and aspirations underpin and determine those choices. During the disabling experience of chronic pain, self-knowledge is dynamic—devolving and evolving as people attempt to accept and adjust within their unsettling, changing life course.24
In identifying unique characteristics of autonomy in rehabilitation care, Caplan et al25 state that coping with disabling injuries and illness during rehabilitation “leaves some patients emotionally unwilling to try and make decisions for themselves even though they retain the cognitive capacities to do so.”25(p11) These authors support “an infringement of autonomy [by rehabilitation professionals] in the short run…during the initial stages of rehabilitation” as a justified harm because patients may be “depressed and demoralized by the severity of their impairments”25(p11) to the point of not being able to participate in decision-making for themselves. Although Caplan et al25 also support the return of decision-making to patients as they adapt to disabilities, the transference of authority is still framed in the medical conception of respecting autonomy that assumes a stable self-knowledge underlying autonomous decision-making.
Supporting Patients’ Dynamic Self-Knowledge
During the rehabilitative process, a stable self-knowledge is not lost and found; self-knowledge changes and develops as patients learn new information and skills and have time for personal reflection and observation.22,24 Dynamic self-knowledge can complicate or thwart a patient’s everyday autonomous decision-making concerning their quality of life, self-care, and self- management that rehabilitation requires. For professionals, the moral challenge to respect patient autonomy during rehabilitation is not simply allowing and granting the transfer of decision-making authority as patients recover. Their moral responsibility lies in supporting the dynamic self-knowledge of patients that empowers autonomous decision-making in consideration of the values, beliefs, relationships, and aspirations within their lives.
Nancy K. Schlossberg’s transitional model in adult development theory helps clarify the concept of dynamic self-knowledge and elucidates how autonomy is a process that takes time and may occur in an ebb-and-flow manner.26 Schlossberg’s model incorporates both anticipated and unanticipated transitions in a person’s life course. Life transitions, whether positive or negative, change the “individual’s roles, relationships, routines and assumptions,”26(p38) leaving them confused and “adjusting to discontinuity.”26(p3) According to Frederick Hudson, transitions are “a natural process of disorientation and reorientation that alters the perception of self and world and demands changes in assumptions and behavior.”27(p96)
Life Transitions
People living with chronic pain experience several life transitions:
- Because the experience of chronic pain begins with an unanticipated bodily insult through illness or injury, a person first encounters a life transition to that of a person in pain.
- When they turn to healthcare professionals, hopeful that medical science will relieve their pain, they transition to being a patient.
- When medical science is not able to cure their pain, they face another unanticipated transition struggling to cope and adapt to the disabling experience of chronic pain, often without adequate and timely help from healthcare professionals.28
- They learn and adopt strategies that are often maladaptive, negatively impacting their relationships and life plans.
- Additionally, mental health issues and addiction may become factors in their disabling experience of chronic pain.
When the experience of chronic pain continues to be a struggle without positive results, multidisciplinary programs are an important treatment option for people to consider.
Entering a multidisciplinary program, people living with chronic pain begin the rehabilitation process as an anticipated transition in their life. Although the transition to acceptance and self-management of their pain is positive and anticipated, it is still another evolution in their life course that will require “adjusting to discontinuity … [because] old strategies no longer work.”26(p3) The unsuccessful strategies they developed transitioning first to a person in pain and then to a person living with chronic pain must change. The patient is challenged to “uncover their own sources of strength and adaptation”26(p3) in order to learn more about their self and the values and beliefs that make sense in their life and contribute to living a meaningful life.
Evolving Relationships
As the patient’s physical and psychological capabilities change with time and with the progress they make in rehabilitation care, autonomy as situated and relational involves evolving relationships between patients, caregivers, and healthcare professionals.2,27,29 Harold Braswell29 asks, “What kind of relationships cultivate autonomy?”(p86) While this is an important question in the lives of patients progressing through a rehabilitation program, the more pointed and necessary question is, “What is the patient’s relationship with their self?” Their relationship with self grounds their relationships with others and guides their autonomous decisions and choices about their roles, relationships, and life plans. Developing new self-knowledge during rehabilitation, a patient’s relationship with self changes, empowering them in making their autonomous decisions and choices about how to live in the world in new ways.
A conception of autonomy as relational and dynamic is more robust and better suited for enacting respect for patient autonomy in the complex and multi-faceted nature of chronic pain management programs. Within the disorientation and reorientation of transitioning during experiences of chronic pain and its consequences, patients seek help “to perceive and organize their life stories, learn to use and make sense of their experiences, and reconstruct their narratives during a life transition.”26(p55) For patients in rehabilitation, they, and their autonomy, are transforming and growing as they gain self-knowledge and clarity regarding their values and beliefs and reorient the construal of their life.
Frida Kahlo and Dynamic Self-Knowledge
Frida Kahlo illustrates how a person’s self-knowledge and relationships change as they transition through recovering from a major health crisis and cope with disability and chronic pain. While Kahlo was recuperating from the streetcar accident, her parents brought her art supplies to her hospital room and an apparatus was built so that she could draw and paint while lying down.30 A friend remarked that, through painting, Kahlo formed a new identity.31 Interpreting her work, art historian Frank Milner32 notes that she reinvented herself and that her paintings, rather than conveying meaning, are emblematic, “speak[ing] most clearly of herself.”36(p86)
Explaining her multitude of self-portraits, Kahlo claimed, “I am the person I know best.”30(p3) Kahlo painted several early self-portraits against a blank background, but starting with “Self-Portrait – Time Flies,” 1929, she contextualized and situated her remaining self-portraits. In “My Grandparents My Parents and Me,” 1936, Kahlo painted herself within her family as an infant. In her unfinished family painting, 1949-1950, she paints herself as an adult within her family tree. She represented her changing relationship with her husband, Diego Rivera, a prominent Mexican painter. In “Frida and Diego Rivera,” 1931, which was painted around the time of their wedding, they hold hands, but stand apart. In “Diego and Kahlo,” 1944, Kahlo painted them sharing a face, conjoined and inseparable from each other.
Kahlo’s art work, however, expresses more than her relationships with the people in her life. In many self-portraits, she painted backgrounds of vines, leaves, and roots, both literally and metaphorically representing her relationship with nature. She also included her pet birds, monkeys, and dogs in many self-portraits. By creatively symbolizing and depicting her Mexican culture and heritage and her political affiliation with the Communist Party, Kahlo also painted her relationships with landscapes and her socio-political environment.30,42
Through her art, Kahlo conveys her relationship with herself and her relationships with the people, circumstances, and contexts that formed her and influenced her life. She represents her whole person over time making sense of her experiences, decisions, and choices within the “practices, narratives, and tradition”2(p287) of her time and culture, which Rachel Haliburton claims is the basis for situated autonomy.2
Creative Autonomy Through Expressive Therapies
In order to employ a conception of autonomy that is relational, dynamic, and reliant on patient self-knowledge, patients need opportunities to explore, communicate, and integrate their lived experiences of chronic pain and its consequences. Expressive therapies (also called expressive arts therapies or creative arts in counseling) are treatment interventions that use the arts to foster potentiality and possibility. According to Cathy Malchiodi,33 the use of arts for healing and health has a long history and has developed into a psychotherapy and counseling treatment modality. Natalie Rogers, a pioneer in the field of expressive therapies, describes expressive therapy as “non-verbal and/or metaphoric expression [with the ability] to facilitate growth and healing.”34(p2)
Malchiodi defines expressive therapies as “the use of art, music, dance/movement, drama, poetry/creative writing, play, and sandtray within the context of psychotherapy, counseling, rehabilitation, or health care.”33(p2) Each of these creative mediums can be used separately or in conjunction with other mediums as a therapeutic technique. However, collectively they constitute their own distinctive domain as a means of “self-expression and…as a language”35(p122) between the patient and the therapist. Although the unique therapies have similar and different goals,33 they all are active processes that reflect a dynamic, therapeutic style that promotes personal change, which is essential for patients caught in the web of the experience of chronic pain and its consequences.
Action and Verbal Expression
The therapeutic basis of expressive therapies is a synthesis of action expression and verbal expression. The patient engages in a non-verbal process of active self-expression via their imagination to create a project. The creative project furnishes “access to whatever might be in the vast reservoir of the unconscious so that [patients] can break through habitual patterns of perception, thought, and behavior, a goal central to all therapy.”36(p81) Using “verbal reflection about the product or experience,”33(p10) the expressive therapist works to guide patients “toward understanding, respecting, and integrating as much of themselves as possible.”36(p81) The active engagement of creative practices enables patients who are negatively affected by the daily sensory experiences and limitations of chronic pain to perceive their potential for making new, positive, and meaningful changes in their lives.
Five Stages of Change
Expressive therapies can be used to intervene at any of the five stages of change—outlined by Kerns et al37 as precontemplation, contemplation, preparation, action, and maintenance. Holt and Kaiser have studied the benefits of expressive therapies particularly on patient motivation in the early stages of change.38 By gaining self-knowledge about their behaviors and how those behaviors conflict with their values and goals, a patient comes to understand how their behaviors affect others and their social environment. Moreover, patients can recognize alternative behaviors available in their social environment. In addition, the action-verbal synthesis of expressive therapies that leads “to insight and the discovery of new or repressed parts of the self”39(p402) is beneficial during all the stages of change during rehabilitation.
Because expressive therapies promote “thinking in a flexible and exploratory manner,”40(p432) patients reveal and assert their lived experiences differently in each stage of change. Someone in the precontemplation stage of change, where their interest in changing is limited, will express their lived experience differently in a creative project than if they were in the action stage of change where they are actively working to change their behavior. Assisting patients “to recognize the voices from the inside, so they can find their way clearly and negotiate successfully through the hazards and alternate routes along their separate pathways”36(p81) supports self-knowledge and promotes a robust, dynamic conception of autonomy in rehabilitation.
Including expressive therapies in healthcare to foster self-knowledge would be especially fruitful for people living with chronic pain.22,33,41 Providing patients with the access and the means to use a creative, intuitive, and imaginative process to express their lived experiences, chronic pain management programs give patients the opportunity for deeper reflection and meaning-making about their experiences of chronic pain and its consequences. Developing flexible and open-ended thinking skills is “associated with coping skills and positive mental health, as well as resiliency and even happiness.”40(p432) Finding a deeper sense of oneself and a better understanding of oneself through expressive therapies allows patients to develop their autonomy by expressing their chronic pain narratives in their own chosen creative way—by, perhaps, writing poetry or identifying songs that connect to their lived experiences, or choosing to perform a dance practice.
Frida Kahlo and Creative Autonomy
Illustrating creative autonomy, Frida Kahlo firmly knew that she was using her visual art to express her lived experience of chronic pain, declaring: “My art is not from my imagination, but from my reality.”42(p266)Andrea Kettenmann31 remarks that Kahlo’s “works should be viewed as metaphorical summaries of concrete experiences” where “fact and fiction fuse in her works…as two components of one and the same reality.”20 Kahlo juxtaposed the harsh medical nature of her spinal surgery against the background of her native Mexico in “The Broken Column,” 1944. She painted herself standing with one foot in Mexico and one in the United States in “Self-Portrait Along the Border Line Between Mexico and the United States,” 1932. Two paintings, “The Two Fridas,” 1939, and “Tree of Hope,” 1946, are each double self-portraits representing, in the former, her feelings surrounding her divorce and, in the latter, her hopes for recovering from a spinal surgery.
While painting was Kahlo’s primary creative expression, she also used many other expressive arts during her life. Recovering from polio when she was a child, Kahlo participated in masculine sporting activities such as bicycling, boxing, and wrestling, expressing her physical exuberance and rebellious personality.42 As an adult she dressed in traditional Mexican dresses and costumes, making a spectacular, dramatic sight on the streets of major cities such as New York, Paris, San Francisco, and Detroit. She also loved singing and leading sing-alongs of traditional Mexican songs and political songs. One story of Kahlo describes her engaging in dramatic/performance arts. While ill and bedridden after spinal surgery, she contrived puppet shows using her feet. Through all of these creative expressions, she narrated her life in meaningful ways.
Narrative Autonomy as Autobiography
A patient’s story of chronic pain and its consequences may be told in two ways: as biography or autobiography. The medical chart is the patient’s biography as told by the healthcare professionals who treat them.43 The chart records the facts and events of the medical story that professionals identify as significant in rehabilitation care, constructing the patient as the object of the medical chart with their illness as the topic of the story.44 Reflecting the biopsychosocial model, multidisciplinary chronic pain management programs consider and chart many aspects of patients’ lives such as familial relationships, daily living functions and adaptations, the patient’s willingness and compliance with program protocols, and insurance funding and limits. Because of its importance for treatment decisions about healthcare, the medical chart’s focus remains on the story of the patient as told by the healthcare professionals rather than on the patient’s lived experiences of chronic pain.
As a biography, the medical chart is meant to be a valid interpretation of the patient in order to address the patient’s chronic pain with appropriate interventions.45 Yet, it separates the illness from the person and their life story. This separation may be useful for scientific evaluation and determination of interventions; however, a medical chart cannot encompass a patient’s lived experiences.44 It contextualizes the patient’s experiences to specific medical times and places, thus limiting the patient’s story to the medical chart. Chronic pain, along with its associated mental health conditions and possible addiction, is “embodied in a particular life trajectory, environed in a concrete life world.”45(p31) Not only does a patient have a life that holds their story of chronic pain; their story of chronic pain holds their life. Healthcare providers, as biographers, have limited knowledge of this intricate and interdependent connection within a patient’s lived experiences. This limited contextualization is not enough to understand a patient’s autonomous decisions and choices. Professionals in chronic pain management programs need autobiographies to meaningfully interpret and respect a patient’s autonomy.
The Patient’s Voice
One critique of current chronic pain management guidelines by the American Association of Family Practice is that “the patient voice and preferences were not explicitly included.”46 This is problematic because patients are “wounded not just in body, but in voice.”37(pxii) Yet, to improve their physical and mental health, patients who become disabled from an injury or illness that causes chronic pain, and its possible mental health conditions and addiction, need to find their voices and tell their own stories.47 As an autobiographer, “the patient’s attention is focused on [their] self.”48(p5) Professionals need patient autobiographies to meaningfully interpret and respect a patient’s autonomy. According to Roy Pascal, autobiography is both historical and cultural as “an interplay, a collusion, between past and present; its significance is indeed more the revelation of the present situation than the uncovering of the past.”48(p11) Jerome Bruner sees the self in autobiography as both narrator and protagonist, with the protagonist “always…pointing to the future.”49(p121)
Autobiography in Rehabilitation
In rehabilitation, patients can take time to review their life, both past and present, in an effort to understand their experiences of coping with their pain and disabilities. From their unique position, patients relate and interpret their interactions with the facts, events, and circumstances of their life, especially their chronic pain experience.48 By choosing the events to highlight and to relate in telling their own story, patients make meaning of their current life experience. By making autonomous decisions and choices, patients tells their own story, moving forward to transform their relationships to themselves, to others, and to their own life.
“In response to a rupture or turning point in the course of [their] life,”70(p33) patients tell stories as a part of their experience of chronic pain. Telling their stories, patients can make judgments and choices about how to cope in both small and large ways, and how to live with the disorientation of their experiences.45 Telling a story that explains past and present, patients reveal their life’s threads of relationships, emotions, personality, and personal ethics. They try to find meaning in past experiences, make meaning of present experiences, and envision meaning for future experiences.
To tell their stories of chronic pain, patients reconnect their bodies to their selves and their selves to their world, then portray their story “through the body.”37(p2) Using expressive therapies as a transformative therapeutic engagement of the patient with their imagination and creativity, patients tell their stories through the body in a multitude of ways that may or may not require the voice, yet represent the voice. Because expressive therapies “involve the [patient] in the invention of his or her own world”28(p75) and in the development of their internal voice, they are able to re-examine, re-imagine, and re-tell their chronic pain narrative within their life story. Developing knowledge about one’s self and one’s values and beliefs empowers patients in their autonomous decision-making that engenders a narrative voice telling their stories.
Frida Kahlo and Autobiography
Through her lifelong artwork, Frida Kahlo portrayed her autobiography, finding ways to live a life that was meaningful to her and to the world. Although Kahlo’s paintings representing her chronic pain and health problems have received particular attention in healthcare fields,3,4 they are only a small part of her body of work. Through personal creative expression, Kahlo made sense not only of her chronic pain experiences, but also of her life, which has led to her legacy as an autobiographical painter.42 Her body of work tells us her story. She contextualizes and represents her life from her birth scene to her death. She understood herself and creatively expressed her experiences, feelings, and ideas31,42 regarding her relationships, socio-political world, and her connections to nature. Milner32 notes that her “symbolism is…straightforwardly intelligible, usually representing specific autobiographical problems and anxieties.”17 From her creative expressions, we are able to know her and better understand the decisions and choices she made in her life.
In her last signed painting, “Viva la Vida,” 1954, Kahlo ends her artistic career with a painting of watermelons symbolizing both the vitality of life and the certainty of death in Mexican culture.42 The watermelons are set against a setting of blue skies and rich, brown earth. One watermelon is depicted as a whole in smooth, deep greens while another is depicted from its roughened stem-end in exploding greens and yellows. The remaining ones are cut and arranged in assorted positions showing their brilliant red flesh and their vital black seeds. In this celebratory completion of her autobiography, Kahlo portrays life as vibrant and abundant and, with the painting’s inscription, invokes us all to “live life.”42 An autobiography that all patients living with chronic pain should have a chance to tell.
Conclusion
Advancements in pain science will continue to guide treatment interventions in multidisciplinary rehabilitation programs for chronic pain; however, patients in life transitions need time, space, and attention to tell their life stories in creatively transforming ways.2 Hudson27 describes living creatively during transitions as “collaging your way through time and space. You arrange and rearrange your colors and shapes as you move along. You pick and choose, search and find, wander and get lost, cut and paste—assembling and disassembling yourself and the universe around you.”(p202-203) Reframing autonomy as a relational-creative-narrative conception allows for situated and dynamic selves that are changing, growing, transforming. By participating in a creative process during their life transitions in rehabilitation, patients gain new knowledge about themselves and their values and beliefs that informs their autonomous decisions and choices as they express and integrate their chronic pain experiences within their life story.
A relational-creative-narrative conception of autonomy also opens the way for healthcare professionals to fulfill their moral responsibility regarding their patients’ autonomy. By encouraging and supporting their patients’ narratives of chronic pain experiences within their life stories, they promote, rather than simply respect, patient autonomy. Chronic pain management programs meet the moral dimensions of their patients’ care by including expressive therapies interventions as an opportunity for people living with chronic pain to make sense of their experiences, develop new self-knowledge, and to tell their life stories.
The meaningful exercise of autonomy is an important goal of healthcare ethics. Examining autonomy in a rehabilitative setting allows for a reframing that can be expanded to all healthcare settings. A relational-creative-narrative conception of autonomy throughout healthcare promotes a more robust consideration of patients’ changing relationships, their creative responses to life transitions, and their life stories, that is, their dynamic autonomy.
I would like to thank the Journal of Humanities in Rehabilitation reviewers who gifted me their time, energy, and expertise which expanded my research and improved the writing of this article.

![]()
This work is licensed under a Creative Commons Attribution 4.0 International License.
United States Military Veterans with traumatic brain injury (TBI) typically have other medical conditions such as post-traumatic stress, insomnia, headache, chronic pain, and moral injury. Interdisciplinary care that holistically addresses TBI and comorbidities is a preferred approach to care. One challenge of interdisciplinary care is effective communication between the patient and providers, as well as among the providers themselves. Discipline-specific jargon, while relevant and effective for diagnosis and documentation, potentially creates confusion in communication with patients and colleagues.
The importance of addressing injuries from a holistic perspective is highlighted in this case study, encouraging rehabilitation clinicians to consider incorporating Art Therapy into interdisciplinary care. By expanding the therapeutic lens and developing a broader, deeper, and more humanistic understanding of symptomatology, interdisciplinary care is enhanced.
The Marcus Institute for Brain Health (MIBH) at the University of Colorado provides interdisciplinary diagnosis and treatment of war Veterans with TBI and comorbidities. The Intensive Outpatient Program at MIBH includes neurology, psychotherapy, physical therapy, speech and language pathology, integrative medicine, and Art Therapy, among other medical disciplines.
In this case, a Veteran’s art served as a visual means of communication, powerfully and immediately expressing mental, physical, emotional and spiritual injuries. The Veteran’s art increased his self-awareness while informing the clinical team of his ongoing experience. Art guided and informed clinical care as providers addressed problems such as psychological impairments, laryngeal dysfunction, postural deviation, and manifestations of unprocessed grief and trauma.
This case study shows how a trauma-informed, creative, interdisciplinary approach can improve communications in clinically assessing and treating Veterans suffering from the complexities of military service-related TBI and psychological trauma. The study highlights implementing Art Therapy to aid a Veteran in processing trauma, while also empowering him to use his visual art to communicate to his interdisciplinary therapists in a unique and powerful manner.[/vc_column_text][vc_column_text]
Introduction
Interdisciplinary care (IDC) is crucial to treating Veterans with traumatic brain Injury (TBI) and post-traumatic stress (PTS), because the etiology of symptoms may be impossible to identify and apportion.1,2 A diverse healthcare team addressing TBI and PTS from multiple perspectives increases the likelihood of improved functioning and thriving as a “whole person.”3,4 Interdisciplinary care requires healthcare professionals to address physical, psychological, and spiritual needs. The patient, and when possible the patient’s family, are members of the team.
Art Therapy has been successfully incorporated in military healthcare settings across the U.S. and elsewhere to address physical and psychological injuries of war.5-11 The goal of this paper is to highlight the role of Art Therapy as a component of interdisciplinary care for Veterans with TBI and PTS.
Several studies exploring Art Therapy within interdisciplinary care for TBI rehabilitation have emerged from active-duty military healthcare settings.5,9-12 The National Endowment for the Arts: Creative Forces website is an excellent resource to review research with “key clinical findings indicating that the creative arts therapies can enable recovery from traumatic experiences.”13 This study furthers these previously-published findings by examining the impact of Art Therapy on a Veteran’s interdisciplinary care in an outpatient rehabilitation setting.
The Marcus Institute for Brain Health (MIBH) addresses the complex needs of Veterans with TBI and related psychological disorders. This uniquely-designed program allows for more in-depth behavioral health and integrative approaches than traditional rehabilitation programs.
The MIBH provides interdisciplinary evaluations and treatment using the innovative Integrated Practice Unit (IPU) model, which seeks to “improve patient-centeredness,”14 and allows Veteran to access informed and highly personalized care. The IPU helps avoid silos of specialty care, and organizes healthcare according to patient needs. “In an IPU, a dedicated team…of both clinical and nonclinical personnel provides the full care cycle for the patient’s condition.”15 Art Therapy plays an essential role at MIBH. Therefore, the aims of this case study are to demonstrate how:
- Art Therapy provided a Veteran the opportunity to creatively express himself and expand his participation on the care team by non-verbally communicating his experience of biological, psychological, social, and spiritual injuries.
- Art created by the Veteran informed the care he received from an art therapist, clinical psychologist, integrative therapist, physical therapist, and speech-language pathologist.
Case Description
The individual described in this case was a 34-year old Caucasian Veteran of the United States Army (co-author “MH”). He served as a US Army Explosive Ordnance Disposal Technician and was exposed to numerous blasts during his military service. MH had one combat deployment to Afghanistan in 2014. During that deployment, he sustained his worst head injury, with loss of consciousness from close-range exposure to an explosive device. MH was medically separated from military service with 100% service-connected disability. His health conditions included PTS, TBI, gastroesophageal reflux disease, and tinnitus. He reported depression and anxiety, problems with memory and concentration, chronic fatigue, headache, impairments in coordination and balance, dyspnea on exertion, throat discomfort, photophobia, and orthopedic injuries.
The interdisciplinary team diagnosed multiple mild TBIs, with ongoing neurological sequelae. Post-traumatic stress, including moral injury, was diagnosed by the clinical psychologist. Impairments of visual motion sensitivity, cervical proprioception and reduced efficiency of postural control in eyes-closed conditions with aggravation of symptoms (dizziness and nausea) were identified by the physical therapist. Exercise limitations and throat tension and discomfort, previously diagnosed as paradoxical vocal fold movement, were recognized by his speech-language pathologist. The integrative therapist’s evaluation identified moral injury and unresolved grief from a spiritual perspective. Art Therapy recognized anxiety and the need for trauma processing, increased self-awareness, and emotional regulation.
The Use of Art Therapy to Elicit a Veteran Voice
At the MIBH, Art Therapy targets the treatment goals of reducing anxiety, expressing feelings, gaining insight and self-awareness, improving emotional regulation, and enhancing neuroplasticity.16 After the initial Art Therapy session, specific goals are identified and projects are tailored to each Veteran’s injuries and experiences. Although Art Therapy is a mental health profession, this case describes how MH’s art expressed psycho/social/spiritual themes, and also his lived experience of physical conditions. Data collection for this case study involved photographing MH’s artwork and collecting statements he wrote to describe his art-making process.
Week 1
At the MIBH, Art Therapy begins with a projective technique in which each Veteran creates an abstract ink design, identifies an image embedded in the design, and completes the picture with colored media.17 The art therapist guides the Veteran in verbally exploring this imagery to find meaning. Artwork emerging from this project contains themes often tied to trauma, which informs and helps refine treatment goals. Figure 1 displays MH’s initial inkblot drawing.
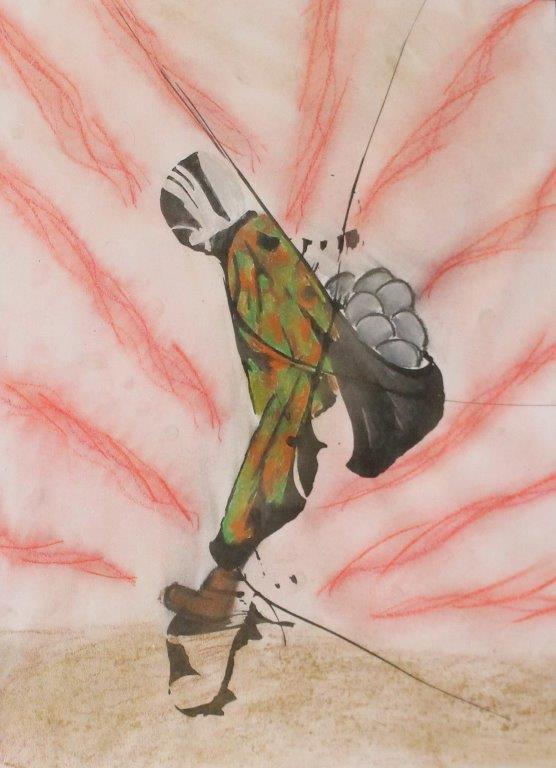 Figure 1. “Burdens We Carry” (ink and chalk pastel)
Figure 1. “Burdens We Carry” (ink and chalk pastel)
Narrative from MH: A nondescript Soldier carries stones, burdens from life and war. Uncomfortable and unstable, the Soldier struggles to gain positive footing but is met with resistance from the weight of the load. Hands are one with the satchel; this burden has become a part of the Soldier. Pain and uncertainty accompany every step; progress is slow to nonexistent. (MH)
Interpretation from the IDC team: Figure 1 illustrated immobilization, both physically and emotionally. MH identified the satchel of stones as a metaphor for guilt, regret, and moral injury that had burdened him for years following repeated traumatic losses. This picture was effective in describing MH’s perception of psycho-spiritual challenges and physical imbalance and restriction.
Week 2
Generally, by the second week of the MIBH Intensive Outpatient Program (IOP), patients are fully engaged in therapy, and artworks shift toward illustrating themes of change. In week two, MH created a small clay sculpture (Fig. 2), based on imagery elicited from eye movement desensitization and reprocessing18 sessions with the psychologist. At this point, MH began requesting additional time in the Art Therapy studio to process changes he was experiencing as a result of care.
 Figure 2. “Removing My Armor” (air-dry clay and mixed media)
Figure 2. “Removing My Armor” (air-dry clay and mixed media)
Narrative from MH: A nondescript warrior removes worn and battle-damaged armor. The warrior has carried this armor for lifetimes and finds it fused to his flesh. Removing this armor is painful and scary but necessary for growth. Like a beetle molting its exoskeleton for growth, so must this warrior put aside his armor. Nature reaches up to assist the warrior, with all things returning to the Earth to be cleansed and eventually renewed. (MH)
Interpretation from the IDC team: Metaphorically “wearing armor” is a common phenomenon of the physical manifestation of stress from traumatic events.19 A guided visualization of releasing symbolic body armor during a psychotherapy session was made concrete in this sculpture. Symbolizing this process with tangible materials provided MH the opportunity to sustain focus on dismantling his armor: a meditative process to visualize change.
Week 3
In the third week, final therapeutic interventions take place. Veterans and IDC clinicians establish closure and follow-up care. In choosing a final art project, MH came “full circle,” returning to the ink-blot technique (Fig. 3).
 Figure 3. “Construction Anew” (Ink and oil pastel)
Figure 3. “Construction Anew” (Ink and oil pastel)
Narrative from MH: Form in chaos. Momentum and energy are moving towards rebirth and growth. A new world is born from removing the barriers and confinement built by self-destruction. Construction is not yet in a finalized form but has purpose and uses new tools. (MH)
Interpretation from the IDC team: MH identified a black raven (center), sunset, water, and mountains in this inkblot. Themes from nature have been identified in Art Therapy research as symbols of healing.5 From a gestalt perspective, and in contrast to the immobilized soldier in Figure 1, this picture resembled a human figure striding forward with fluid movement.
Although MH created other artworks, those displayed here mark important stages in his healing process: (1) identifying problems; (2) visualizing change; and (3) utilizing new skills to empower himself. Reflecting on his Art Therapy experience, MH wrote:
Art Therapy is a remarkable tool that allowed me to access my subconscious and conscious minds. It was an outlet for emotions and self-realizations to be expressed when words failed. Art was the most efficient way for me to show my pain, my barriers, and my progress. Pain is such a specific internal state, difficult to express so others truly understand. I found that using art allowed me [to] express my pain in a universal language. My team was able to observe issues I presented in my art I would never have been able to express in words. Some of these issues were outside my conscious awareness until I processed them through art and received feedback. My burdens and armor had become a part of me to the point where I was unable to separate them from myself. Art Therapy allowed me to access uncomfortable areas in an organic and comfortable manner and maximized my time at MIBH. It is a tool I still use and find comforting and stabilizing in times of chaos and uncertainty.
Veteran Artwork Influencing Clinical Care
Several times a week, the IDC team met to discuss and refine MH’s care. His artwork and comments were presented by the art therapist during rounds. The art therapist identified symbols in the artwork relevant to interdisciplinary therapeutic goals. Each clinician shared observations allowing for the integration of multiple perspectives. This created an improved, holistic clinical understanding and assisted in designing humanistic, person-centered, integrated care. MH’s artwork depicted themes that overlapped disciplines. For instance, artworks describing psychological and spiritual burdens were simultaneously symbolic of physical posturing, pain, and restriction. The collective effect of multiple therapists communicating and treating interwoven symptoms was articulated by MH: “The IOP felt like one continuous session with different components, each offering a unique avenue for healing.” This holistic approach and response may provide a case-level example of successfully utilizing mind/body interventions.20
Each work of art created by MH provided direct communication with the care team, who used their discipline-specific interpretation to direct treatment strategies. Figure 1 illustrated psycho-spiritual challenges related to PTS and moral injury. In psychotherapy, MH explored his belief that carrying emotional burdens was his responsibility, yet these burdens were immobilizing. Integrative techniques based on Eastern medicine conceptualized the spiritual injuries and energetic blockages from trauma recognized in Figure 1. MH needed permission and effective tools to release the guilt and fear he carried. Art Therapy, psychotherapy, and integrative therapy all utilized metaphors embedded in Figure 1 to understand MH’s experience of PTS and moral injury.
The physical stance illustrated in Figure 1 mirrored symptoms identified by the physical therapist and the speech-language pathologist. The physical therapist observed forward head posture and guarded positioning, matching MH’s physical presentation with postural-balance instability. Patterns of muscle tension evident in the drawing mirrored MH’s physical presentation in voice therapy as well. Behavioral habits of breath-holding, over-exertion in physical activity, and musculoskeletal chest and neck tension were addressed by the speech-language pathologist, increasing MH’s awareness of stress and tension in daily life. Diaphragmatic breathing was encouraged across all disciplines for a variety of physical, emotional, and spiritual benefits.
The eye movement desensitization and reprocessing provided by MH’s psychologist helped him recognize the metaphorical armor he had donned for psychological protection, which manifested as tension-holding physical restriction in his upper body. In week two, MH explored the concept of slowly removing this “armor,” with visualization techniques. Art Therapy provided him an opportunity to symbolize removing armor. A detailed, nuanced description of this process appears in the Veteran’s clay sculpture (Fig. 2). Simultaneously, “removing armor” provided an opportunity in integrative therapy to explore vulnerability, a necessary step toward healing spiritual wounds. A practice consisting of mantras and yoga, focusing on the solar plexus energetic center, was initiated by the integrative therapist. According to Eastern medicine, the solar plexus is located in the abdomen, where armor was being dismantled in the sculpture.
The speech-language pathologist also focused on the abdomen, promoting diaphragmatic breathing and relaxation, and demonstrating that body tension and strain had limited MH’s physical performance and vocal function.21 From a physical therapy perspective, this sculpture signified a shift in posture and movement, with the figure appearing strong, centered, and physically grounded.
In week three, MH continued to struggle with self-acceptance and worthiness. Psychotherapy incorporated visual and kinesthetic metaphors to develop internal and external resources. Integrative therapies provided introspective work, visualizing the release of spiritual burdens, reducing the need for protective defenses. These interventions helped MH embrace the freedom expressed in Figure 3.
From the physical therapist’s viewpoint, a gestalt view of Figure 3 resembled a figure running. This interpretation was congruent with MH becoming more physically active and striding forward in life, using new tools to progress further in the future. The speech-language pathologist observed that Figure 3 expressed releasing internalized strain. The heavy figure portrayed in Figure 2 transformed to embody weightlessness, fluidity, and ease in Figure 3. The team observed a transformation in MH’s art, from protective and imbalanced in week one, to open, free, and forward-moving in body, mind, and spirit in week three.
An intriguing element of this case is the rich clinical discussion that resulted from the art therapist inviting all clinical providers to recognize visual symbols relevant to diverse and overlapping therapeutic goals. Additionally, art provided a language and a tool for synthesizing the internal and external changes MH was experiencing in treatment. Art Therapy was satisfying and beneficial for MH, and offered a visual, universal language to communicate his unique experience of injuries and healing to his IDC team.
Conclusions
This case study demonstrates how Art Therapy was an essential element of an IDC team treating a Veteran with TBI and PTS. The study examines how the Veteran used Art Therapy to assist in recovery from traumatic experiences and how his artwork informed the IDC team. Art Therapy is a promising component of TBI rehabilitation that merits further study and application. A limitation of this study is that MH’s experience may not generalize to other injured Veterans receiving Art Therapy. Further research is needed to explore the effectiveness of Art Therapy for TBI and PTS, and to examine specific outcomes of Art Therapy in patients receiving IDC.


Molding a Crisis Curriculum
My initial instinct was to begin with the rich visual history of images depicting outbreaks of the plague from the Medieval and Renaissance periods to the activist art of the AIDS epidemic in the late 20th century, and apply art history skills—learning to read an image or object and analyze it within a social and historical context of its time. Confident that this was a great way for students to learn from the past to better understand our present situation, I began to prepare assignments that probed social and economic inequities of public health crises. I planned to start with a close reading of the chaotic scene of death of all social classes depicted in Pieter Bruegel the Elder’s painting, The Triumph of Death (1562) (Fig. 1) in relation to excerpts from Giovanni Boccaccio’s The Decameron (1351). In this text, Boccaccio described the relative privilege of the wealthy during the 14th-century plague in Florence, noting “the plight of the lower class and, perhaps, a large part of the middle class was even more pathetic,”1 as they did not have the means to leave the city and thus fell sick and died by the thousands. Breugel’s painting and Boccaccio’s text would then be discussed in relation to Nicholas Casey’s article, “College Made Them Feel Equal. The Virus Exposed How Unequal Their Lives Are,”2 to bring the discussion of economic disparities closer to home. Figure 1: Brueghel, Pieter the Elder (c. 1525-1569). The Triumph of Death. Ca. 1562. Oil on panel. 1.17 x 162m. Copyright of the image Museo Nacional del Prado / Art Resource, NY.
Additional opportunities for comparison to contemporary issues can be found in The Chronicles of Gilles Li Muisis, a 14th-century French manuscript chronicling Abbot Guilles li Muisis’ description of the plague in Tournai (modern-day Belgium). In this case, students would compare Pierart dou Tielt’s stark illustration (Fig. 2) of the city dealing with the problem of overflow and burial of dead bodies3 to contemporary photographs of mass burials across the world due to Covid-19 in Alan Taylor’s Vanity Fair article, “An Unimaginable Toll.”4
Figure 1: Brueghel, Pieter the Elder (c. 1525-1569). The Triumph of Death. Ca. 1562. Oil on panel. 1.17 x 162m. Copyright of the image Museo Nacional del Prado / Art Resource, NY.
Additional opportunities for comparison to contemporary issues can be found in The Chronicles of Gilles Li Muisis, a 14th-century French manuscript chronicling Abbot Guilles li Muisis’ description of the plague in Tournai (modern-day Belgium). In this case, students would compare Pierart dou Tielt’s stark illustration (Fig. 2) of the city dealing with the problem of overflow and burial of dead bodies3 to contemporary photographs of mass burials across the world due to Covid-19 in Alan Taylor’s Vanity Fair article, “An Unimaginable Toll.”4
 Figure 2: Miniature by Pierart dou Tielt,Chronicles ofGilles li Muisis (Tournai, c. 1353). The People of Tournai Bury Victims of the Black Death. ms. 13076-13077 fol. 24v. Bibliotheque royal de Belgique.
Another image from the same manuscript, called The Strasbourg Massacre (Fig. 3), highlights a brutal lesson from history—the desire of some groups to assign blame and malicious intent to the spread of the disease. In this case, Christians accused Jews of the purposeful spread of the plague by poisoning water sources, ultimately leading to the extermination of entire Jewish communities.5 While these images are painful to look at and learn about, they provoke compelling discussions on bigotry and intolerance when compared to contemporary conspiracy theories and overt racism toward Asian communities, particularly the Chinese, regarding the origin and spread of COVID-19. This is the power of art history; we can read about catastrophic events and the horrific failings of humankind, but seeing the images packs an emotional punch and promotes a profound reckoning of just how little human nature has changed. Learning to read these images critically and contextually gives students the knowledge and tools to challenge current social, racial, and economic disparities in our current pandemic.
Figure 2: Miniature by Pierart dou Tielt,Chronicles ofGilles li Muisis (Tournai, c. 1353). The People of Tournai Bury Victims of the Black Death. ms. 13076-13077 fol. 24v. Bibliotheque royal de Belgique.
Another image from the same manuscript, called The Strasbourg Massacre (Fig. 3), highlights a brutal lesson from history—the desire of some groups to assign blame and malicious intent to the spread of the disease. In this case, Christians accused Jews of the purposeful spread of the plague by poisoning water sources, ultimately leading to the extermination of entire Jewish communities.5 While these images are painful to look at and learn about, they provoke compelling discussions on bigotry and intolerance when compared to contemporary conspiracy theories and overt racism toward Asian communities, particularly the Chinese, regarding the origin and spread of COVID-19. This is the power of art history; we can read about catastrophic events and the horrific failings of humankind, but seeing the images packs an emotional punch and promotes a profound reckoning of just how little human nature has changed. Learning to read these images critically and contextually gives students the knowledge and tools to challenge current social, racial, and economic disparities in our current pandemic.
 Figure 3: Miniature by Pierart dou Tielt,Chronicles ofGilles li Muisis (Tournai, c. 1353). The Strasbourg Massacre: Jews Burned to Death in Strasbourg during the Black Death, ms. 13076-13077 fol. 24v. Bibliotheque royal de Belgique.
Figure 3: Miniature by Pierart dou Tielt,Chronicles ofGilles li Muisis (Tournai, c. 1353). The Strasbourg Massacre: Jews Burned to Death in Strasbourg during the Black Death, ms. 13076-13077 fol. 24v. Bibliotheque royal de Belgique.
Choosing a Healing Approach
And yet, as I planned these new class sessions charged with critical comparisons to social and public health issues of the current COVID-19 crisis, I wasn’t prepared for how difficult it was to analyze graphic images of death, disease, and massacres, along with heartbreaking images of loss, sorrow, and mourning while living through an actual pandemic. I quickly realized that if the material was hard for me to digest in my own state of anxiety during the pandemic, I couldn’t impose this content upon my students. Recognizing certain methods would not serve my students at this time, I put aside my need to demonstrate the critical rigor of my discipline and revised the rest of the semester to focus on the study of art as a powerful instrument for healing, comfort, and joy. That said, I didn’t throw away my prior work; I will use this material in class at a less stressful time. In fact, after reflecting on the role of the humanities in recognizing the importance of dealing with the unknown, I decided to acknowledge my own uncertainties and share this experience with my students. In our first remote class, I told my students the story of my initial plans, showing them plague images as examples and described my plans to use these works of art to think critically about our current situation. I acknowledged my own struggle with the material and my decision to focus instead on the healing component of art. I shared that my course goals had shifted; I now wanted students to understand how art can provide healing, comfort, and humor in addition to illustrating the inequities of its time. With this in mind, I divided the remainder of the course into three modules on the following topics: Art and Personal Health, Art and Public Health, and Art in a Time of Crisis. As a health humanities scholar, I also applied some of Peterkin and Skorzewska’s key goals for health humanities in postgraduate medical education to this undergraduate course: providing a unique space to question, analyze, and critique contemporary practice while at the same time encouraging self-reflection and cultivating skills of reflexivity, in order to foster a greater understanding of the human condition.6 The following is a brief description and list of some resources used in these modules.Art and Personal Health
In this first section of the course, I assigned short and easily-accessible readings introducing the concepts and studies that demonstrate that looking at art and visiting an art museum benefits one’s physical health, mental health, and emotional intelligence. Students were asked to read and reflect upon these studies, and follow up with a “lab experiment”—a virtual visit to the Metropolitan Museum of Art’s (the MET) Temple of Dendur (via their MET360 project) in order to examine and reflect upon their personal response while viewing art in the midst of a pandemic lockdown. For most of my students (undergraduate non-majors, taking the course to fulfill a core requirement), this was the first time they heard of or even thought about these ideas connecting art and health. I knew I was on the right track when their written responses contained exclamations of surprise, wonder, requests for more information on certain studies, and an overall reaction of finding joy and peace while virtually wandering through the MET, a museum most had never visited in real life. Resources:- Why Going to an Art Museum Could Be as Good for You as Exercise
- Doctors to Prescribe Museum Visits in Pioneering Treatment
- Study Finds Med Students Who Make Time for Art Have More Empathy
- Researchers Have Found That Visiting Art Museums Can Offer Significant Relief for People Living With Dementia
- Visit NYC’s Metropolitan Museum of Art’s Egyptian Temple of Dendur via The Met 360
Art and Public Health
In this section, students investigated the connections between public art and public health. La Salle University in Philadelphia, PA is home to one of the most impressive mural arts programs in the country. We focused on Mural Arts Philadelphia (MAP) and their Porch Light initiative. Students considered Porch Light’s core message to “[work] closely with communities to uplift public art as an expression of community resilience and a vehicle of personal and community healing.”7 In a series of short, accessible readings and a video, students learned about the connection between public art and public health outcomes, and, more specifically, the effects of the Porch Light program on communities in Philadelphia. The Yale School of Medicine studied the impact and health outcomes in Porch Light communities and found increases in social cohesion and trust among neighbors, decreases in stigma toward individuals with mental health or substance-abuse issues, and an increase in the quality of the walking environment and perceptions of safety.7 After a written assignment reflecting on the connection between public murals to community health and wellness, students were asked to create their own “Art & Public Health Mural Arts Tour.” Using the Mural Arts Philadelphia website as their source, students created a PowerPoint tour with images, maps, and accompanying text, explaining why they picked a specific mural and how it related to community health and well-being. Their final slide involved a short critical thinking piece with the following prompts: How much did you know about Mural Arts Philadelphia before this assignment? How much did you know about Public Health concerns? Has this assignment changed the way you think about the role of city murals? Will you look at or interact with them differently? How so? Resources:- Public Art as Public Health
- The Porch Light Initiative Video – Community Healing Through Art
- Philadelphia Mural Arts: Porch Light Program
- Mural Arts Philadelphia website
Art in a Time of Crisis
Having set up an introductory framework on the research connecting art and health, the final summative assignment of the semester allowed students to apply what they learned to their own interests. This project was inspired by the phenomena happening in the creative world at that moment, where artists (and musicians, actors, writers, poets, etc.) were making their work public and free for all to provide joy, comfort, and entertainment during the global shutdown. The primary question of inquiry for this assignment was: what kind of creative work is being made and shared publicly right now while we are in lockdown and the world is reeling from fear, anxiety, and grief? Their task was to search their social-media communities to curate their own exhibition of art (defined in a broad sense) made in response to COVID-19 that offered some form of respite. The narrative accompanying their selections had to connect to the ideas and concepts discussed in the previous two modules with these prompts: Why did you select this creative work? How does this work of art relate to personal health, wellness, or public health? I shared my own list as a model for the assignment: Amplifier’s Free Downloadable art celebrating first responders and public health messages, The Getty Museum Challenge recreating famous works of art, Yo-Yo Ma’s Songs of Comfort, Lin Manuel Miranda & Andrew Lloyd Weber’s “Play-off” on Twitter, and Couple in Lockdown Create Tiny Art Museum for Their Gerbils, and noted that these examples in some way created a “biographic picture” of my interests and personality that I typically don’t get to share with students. Their exhibits were fabulous, with subjects ranging from street art, tattoos, video-game imagery, comics, poetry, songs, and concerts, to many funny and moving TikTok videos. The results were wonderful, and a joy to grade (a somewhat rare experience at the end of a semester).Reflections
This final project allowed me to get to know my students (and they me) on a level that would not have happened in the typical face-to-face classroom environment, which is contrary to traditional thinking about online teaching but makes sense when considering the nature of art. Sarah Blanton, Editor-in-Chief of JHR, noted in her Spring 2020 editorial that through art, “we find that connection of shared experiences, and perhaps we see each other a little more clearly, more compassionately.”8 This class made me rethink how I teach, and what I teach in the introductory course. The unexpected switch to remote teaching forced me to think about content and assessment in ways that I had not considered before. I struggled to leave behind traditional art history methods (visual analysis and critical social/historical studies) to embrace projects that involved studying art as “simply” a form of joy and comfort beneficial to one’s health. This resistance comes from a long history of art historians having to defend and explain the rigor and methods of the discipline to others, particularly in the medical humanities, where the arts can be pigeon-holed as a vehicle for empathy and therapy. I now realize my reluctance was limiting to myself, but more importantly, to my students. I found that there is time for both rigorous methods and compassionate, joyful pedagogy. As a result, these students left my class with more than the typical set of art history skills, just as I left class with a better set of teaching skills. It is Blanton’s idea of art as a method of seeing each other more compassionately that stays with me as I prepare for my Fall 2020 courses in light of the continuing pandemic and the additional public health crisis illuminated by the Black Lives Matter movement. I am planning modules for my students to engage with art critically, culturally, to have the difficult discussions, and to see each other more compassionately. Once again, I will use art as a means of addressing and interrogating issues of health and social injustice, using murals like Eric Okdeh’s The World to Come (Mural Arts Philadelphia, forthcoming, 2021) (Fig. 4) to encourage the trajectory of discussion, understanding, activism, and the ultimate goal: change. Figure 4: Eric Okdeh, The World to Come, (forthcoming Mural Arts Philadelphia, 2021) Eric Okdeh Instagram: @okdehmurals
Figure 4: Eric Okdeh, The World to Come, (forthcoming Mural Arts Philadelphia, 2021) Eric Okdeh Instagram: @okdehmurals 
![]()
This work is licensed under a Creative Commons Attribution 4.0 International License.
[vc_row content_placement=”top”][vc_column][vc_custom_heading text=”DPT Program Stages an Art Show: Using Art to Develop a Heart for the Profession of Physical Therapy” font_container=”tag:h1|text_align:left|color:%231e73be” use_theme_fonts=”yes”][vc_custom_heading text=”By Susan G. Klappa PT, PhD | Yvonne Beth Alles DHA | Scott P Klappa MS” font_container=”tag:h4|text_align:left|color:%23000000″ use_theme_fonts=”yes” css=”.vc_custom_1539545427314{padding-bottom: 30px !important;}”][vc_column_text] Download the article (pdf)[/vc_column_text][vc_row_inner][vc_column_inner width=”1/3″][vc_column_text]Susan G. Klappa PT, PhD*
Download the article (pdf)[/vc_column_text][vc_row_inner][vc_column_inner width=”1/3″][vc_column_text]Susan G. Klappa PT, PhD*
(Corresponding Author)
Professor, Physical Therapist
Briar Cliff University
Doctor of Physical Therapy Program
3303 Rebecca Ave.
Sioux City, IA 51104
Email: Susan.klappa@briarcliff.edu
Phone: 651-335-9813[/vc_column_text][/vc_column_inner][vc_column_inner width=”1/3″][vc_column_text]Yvonne Beth Alles DHA*
Associate Professor
Allied Health
Kent Intermediate School District
Grand Rapids, Michigan
7080 Byron Center Ave.
Byron Center, MI 49315
Email: eayalles88@gmail.com
Phone: 616-878-4494[/vc_column_text][/vc_column_inner][vc_column_inner width=”1/3″][vc_column_text]Scott P Klappa MS
Clinical Counselor
Lifespan
Burnsville, MN
Email: spklappa@gmail.com
Phone: 952-322-0427[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_column_text]There was no grant support for this work.
The IRB at the Davenport University approved the protocol for this study as exempt.
*Formerly from Davenport University
[/vc_column_text][vc_custom_heading text=”Abstract” font_container=”tag:h4|text_align:left” use_theme_fonts=”yes”][vc_column_text]Background: As part of a capstone course, Doctor of Physical Therapy (DPT) students created visual art projects to gain a deeper understanding of how physical therapy (PT) transforms society and improves quality of life for patients. These creative works were displayed in a public art show to engage and educate the community about PT. The purpose of this study was to examine the influence of an art show on professional beliefs of DPT students and on the local community’s understanding of the physical therapy profession.
Methods: Community-based participatory research (CBPR) methods incorporated phenomenological methods to examine lived experiences of DPT students staging an art show and the audience of attending community members. Students completed a questionnaire (n= 40) about their experiences and community members reflected in a journal guest book (n = 30). Data were analyzed for common themes and coded into categories.
Results: Students reported initial skepticism about the art show. The art experience was challenging, but helped students confirm a calling to the profession. Students reported learning new ways of thinking and communication through art to promote the PT profession. The community members reported gaining a better understanding of PT as a profession and feeling a deep connection to PT through the art show.
Conclusions: Art provides opportunities for creative and unique perspectives of thinking about familiar subjects. The PT art show provided students with new ways to problem solve and alternative methods of expressing the essence of their beliefs about transforming society. The community learned about the work of physical therapists through these creative projects and both students and community members were surprised by the power of art to connect them.
Key Words: physical therapist education, art show, community
Funding Source: None
[/vc_column_text][vc_column_text]
Introduction
All healthcare professionals, including physical therapists (PTs), encounter human suffering in their everyday practice as healers. Human suffering can raise fundamental questions related to health, wellness, illness, disability, life or death, and grieving. These questions challenge practitioners who have been educated on behavioral objectives based on traditional cognitive, psychomotor, and affective domains of learning1 to provide adequate and compassionate care for their patients and families. To make situations more challenging, PTs may encounter ethical dilemmas when dealing with patient-practitioner interactions within the healthcare system.2 Physical therapists need to respond properly to situations involving ethical issues as well as manage the distress characterized by human suffering. Traditional classroom environments where the skills and science of physical therapy are taught often fall short in pedagogy to engage students in the three domains of learning (cognitive, affective, psychomotor) within the clinical context.3 Students may cognitively understand how to physically respond to difficult situations but the deeper connection to the heart of distress, and how to respond, often cannot be taught through traditional pedagogical processes.
Medical humanities (MH) and health humanities (HH) are tools to help students develop the ability to communicate about difficult topics while also nurturing skills of observation, creativity, imagination, intuition, empathy and self-reflection, all crucial to holistic practice in healthcare.4-17 Defined by Hurwitz in 2003, MH involve the use of literature and the arts as a means of exploring and discussing human issues pertinent to the health professional.18 The term HH has been coined to represent a broader, more inclusive population of health professionals rather than just those studying medicine.19 This study examines the influence of an art show on professional beliefs of students and on the local community’s understanding of the physical therapy profession. Two hypotheses guided the questions for this investigation: 1) Doctor of Physical Therapy (DPT) students involved in the HH through visual arts will demonstrate a greater understanding of how physical therapy may transform society; and 2) community members will obtain a greater understanding of how physical therapy improves the human condition through the experience of an art show.
The American Physical Therapy Association (APTA) developed a new vision statement in 2013, stating physical therapists are active in “transforming society by optimizing movement to improve the human experience.”20, 21 Principals involved in this new vision statement were meant to inspire the profession and members of society. Eight guiding principles inform the APTA vision statement: identity, quality, collaboration, value, innovation, consumer-centricity, access/equity, and advocacy. Vision statements regarding a deeper connection to society are lofty, but they often beg the question: How does a profession bring that vision to reality and connect with society?
Background
The study and exploration of art in general and the liberal arts more specifically provide a deeper connection to the human experience or condition.4-19 Liberal arts preparation has been viewed as both a necessary prerequisite and an unessential hurdle or relic in the preparation of healthcare professionals. Nevertheless, liberal arts are often a part of prerequisites into entry-level healthcare professional programs and are often neglected once the professional studies commence.4,6-8,11,13,15,17,18 Exposure to the liberal arts as a prerequisite is not enough. Pierce13 suggested liberal arts are a necessary component in the journey to competence as a healthcare provider because they enhance reflective practice skills by providing a structure for reflection. Pierce believed the study of the liberal arts helps students and professionals meet expanded roles as professional and societal citizens through a deeper connection to the human experience. Chomsky22 argued that individuals learn more about the human condition from the arts than from scientific literature alone. Perakis12 suggested while the arts in general may be both disturbing and eye-opening, visual images are powerful and catalyze change. As students examine their role in society from a professional perspective, engaging in HH through the visual arts provides an avenue to address reactions to human suffering. The visual arts provide an initiation to a deeper understanding of the human condition through focused self-reflection and personal transformation.6, 7, 11-15, 17,19
While discourse regarding holistic training of physicians and other healthcare professionals has embraced the pedagogy of HH, curricular inclusion of humanities in health professions has been both encouraged and debated.3-19 Proponents of HH claim inclusion of the arts in medical education, for instance, provides medical students with a greater ability to extract meaning from lived experiences17 and an ability to connect with shared human experiences.6-9, 11,12, 14, 15-19 Respect for individual differences, an enriched use of language, and expanded appreciation of others’ perspectives and lived experiences also occur as a result of exposure to HH and the visual arts.16 Smith et al15 suggest that including HH in the training of health professionals results in a deeper appreciation of the complexity of human experiences, a greater sensitivity to individual differences, and a more nuanced understanding of illness, suffering, dying, and grieving. Smith et al15 further suggest that students involved in HH gain a greater ability to make deeper connections between personal and professional knowledge when dealing with situations infused with grief. Perakis12 suggests that students exposed to HH are better equipped to deal with suffering and afflictions of those they serve. Students also possess more sophisticated expressive and observational skills as a result of HH and art-based learning.8,12,14,15 Creating and experiencing visual art provides holistic techniques for deep self-reflection and allows access to sharing lived human experience in ways not possible through traditional discussion groups, patient simulations, written papers, or presentations.14
Insights from HH allow students and the community to view lived experiences from the eyes of the other and gain new ways of seeing possibilities for reaching full participation in life roles.6 Middleton and Drucquer11 discuss using an artist’s view as a means to approach patients through multiple lenses to adapt to challenging situations. The artist’s view may allow the healthcare practitioner to demonstrate improved human interaction and better pattern recognition skill when diagnosing patients. In addition, the visual arts can aid in self-care of the practitioner. After a long day of stress, patient-practitioner interactions and strategies of engaging with visual arts may lead to improved coping skills.11 Kirklin et al8 suggest that visual arts-based observational skills correlate to improved observational skills of doctors and nurses in determining when to refer patients with skin lesions to dermatology, thus ultimately improving patient-practitioner relations and overall care. Macnaughton10 suggests that the healthcare practitioner as artist seizes an opportunity for greater creativity in providing care, improving the human condition of both the patient and the practitioner.
The marriage of science and art is not new. In his history of medicine, Porter23 points out that the ancient Greeks emphasized the common ground between philosophy, medicine, and ethics. With the increased emphasis on evidence-based practice in physical therapy and medicine, the humanities and arts have been relegated to a lesser position. Yet, the essence of the patient and practitioner experiences may not be measured solely through numbers using positivistic approaches to research.24-28 The artist’s view of the world emphasizes common ground in society by providing insights into fundamental issues regarding human existence, including death and dying.11 The visual arts provide the community with a stage to learn about a profession and possibilities for improved function and transformation.
While there is much literature on the use of HH in the preparation of physicians, nurses, occupational therapists, and others such as emergency medical technicians, a paucity exists regarding the role the visual arts might play in physical therapist education. There was also no evidence in the literature about how the visual arts influenced the education of the community on the roles of physical therapists. This study attempts to fill those gaps in the literature.
Methods
To address the purpose and hypotheses of this study, community-based participatory research (CBPR) methods incorporate a phenomenological survey to examine lived experiences of DPT students staging an art show and community members attending the show. CBPR involves “a commitment to conducting research that shares power and engages community partners in the research process and benefits the communities involved, either through direct intervention or by translating research findings into interventions and policy change.”29 (p.4-5) More than a collaborative approach, CBPR involves building trust and sharing power through all phases of conceptualizing the research problem, conducting research, and disseminating findings.29 All parties learn from the process. Results from a CBPR project may not necessarily be disseminated as a peer-reviewed research paper, but may also take on some other form of education within the community.
For this research project, the DPT program was approached by the university to consider ways in which the university and greater community might learn about the physical therapy program at the university. A professor in the DPT program had preliminary discussions with an art professor who was planning to host an art show in the fall. A partnership was formed between the DPT program, the university, and the greater civic community resulting in an opportunity for the DPT program to share the message of physical therapy identity with the community through the shared time and space of an art show. An opportunity for the DPT program to display visual art describing the intersection of the International Classification of Function (ICF) model and the new APTA vision statement was established.
Phenomenological methods were used to explore the lived experiences of physical therapist students who staged the art show as part of a capstone experience in a DPT curriculum and the experiences of community members who attended the art show. Phenomenological research is qualitative in nature and examines lived experiences to derive meaning from those experiences.24-28 In this process, researchers attempt to set aside personal experiences and biases to understand trends that develop from the lived reality of research participants. Author van Manen defined phenomenology as “the study of the lifeworld or our everyday experiences and the meanings we construct from our experiences.”24(p. 33) Two main assumptions in phenomenological research are: 1) humans seek meaning in their lives; and 2) multiple realities exist that are socially constructed.24-28
Procedures
The study was approved by the IRB with exempt status at Davenport University in Grand Rapids, MI. Inclusion criteria included being a DPT student enrolled in a Critical Integration course in the last year of the DPT curriculum in a Midwestern university. For community members, inclusion criteria included being in attendance at the art show. Adding comments to the reflective journals implied consent of the community members and no names were recorded.
Participants
A sample of convenience was used in this study. After staging the art show, DPT students (n=40) were invited to write confidential reflective papers about the experience of creating art as part of the curriculum in the DPT program. Community members (n=30) from the local university and civic community were invited to attend the art show through a newspaper announcement and university communications. These community members had the opportunity to reflect on thoughts, feelings, and lessons learned about physical therapy as a result of attending the art show. Table 1 lists the type of visual art on display by medium and title. Reflective writing prompts for students and community members are listed in Table 2.
Table 1: Types of Visual Art & Titles
| Photography (12) Community Wellness Who are Physical Therapists? Triathlon: Community Integration Thinking Within the Lines of Therapy Waiting for Some PT Fun Playing with Two Left Legs Value of PT Healing Hands Wrecked Pride and Passion A Leg to Stand On Dignity and Mobility Regained |
| Pen/Chalk Drawings (14) PT Progression It’s not Therapy if it’s not Physical Recovery to Your Potential Journey from Pain to Wellness Layers of Motion The Art of Helping Others Physical Therapy Across the Lifespan Bones Helping Each Other Up A Walk to Remember It Starts from the Ground Up Capturing Movement Physical Therapy Gets Results Equine Therapy: Riding through Life as a Quadriplegic |
| Paintings (4) Physical Therapy Heavenly Hands The Viscosity of Life Breath and Movement |
| Sculptures (6) Tools of Change PT: A JOINT Effort “Progression Highway” Rock Hard Proporzionale Improving Quality of Life |
| Collage/Mixed Media (1) Hands |
| Video (1) Art in Motion |
| 3D Interactive Media (2) Flipping through Rehab (Flipbook) The Allure of Human Movement, a Haiku (Calligraphy) |
Table 2: Reflective Writing Prompts for DPT Students and Community Members
| DPT Student Reflective Writing Prompts |
| What were your thoughts when you first heard you had to create a piece of art to represent the intersection of the ICF model and the new vision for PT (Transforming society through optimizing movement to improve the human experience)? |
| What were your thoughts when bringing in your art to display? |
| How did you feel as we were staging (setting up) the show? |
| How did you feel on the day of the art show? |
| What was it like to have people view your work of art? |
| What did you learn about yourself through this process? |
| What did you learn about your classmates? |
| What do you believe the community learned about PT? |
| Community Member Reflective Writing Prompts |
| What did you learn from the art show experience? |
| How did the art show make you feel? |
Table 3: Themes and DPT Student Comments on the Art Show
| Challenging Assignment – Skepticism Followed by New Ways of Knowing |
| At first I was a little surprised that we would have to do an art project. The thing that really worried me was there wasn’t any specifications that were required. I have done art shows before but they were for an art class and the teacher usually had some kind of specifications for the show. So, I was a little worried about what I should do. I usually make drawings of realistic things so coming up with a concept on my own was going to be a challenge. *P4 |
| My first thoughts of creating a piece of art were, “why are we making art in PT school?” When I was younger, art was one of my favorite classes, but I lost touch with the importance of the class as I progressed into middle school and art school. Then when in undergraduate studies, I took an art appreciation course that put me to sleep. At this stage of my development, I never thought I would complete another art course, thus, explains the reasons why I had mild levels of anxiety about this class project. After being in slight denial of this art project, I began to churn some ideas in my brain about what I could create as piece of art that was meaningful. *P15 |
| I enjoyed the art project and I am appreciative of the opportunity. I think it was hard to initially get motivated for it because, as third years, we are very singularly motivated by the thought of taking and passing the boards. Ultimately this was a nice break in the curriculum that allowed some fun to be had. *P36 |
| Art: A New Way to Communicate |
| I learned that this was a very challenging task for me. I thought it would be easy, but it was not. It was hard to engage my brain to be creative. I have been focused on the other side of my brain for three years and hadn’t had to use my creative skills. While it was challenging to me to create this painting I found it very rewarding and learned that I need to use my creative side more than I do. *P12 |
| I think the community realized that we are creative minds and not just “scientists.” I think health professionals are usually seen as rigid and not creative, but I think they saw that we can think outside the box. I think this was a great opportunity to see a different side of PT and ourselves and very thankful we had the privilege of doing this project. *P25 |
| It was exciting to have people look at our art work, especially those who don’t know what physical therapy is. It seems like they got a great representation of what we cherish and enjoy about our profession as well as the struggles we face. *P32 |
| Lessons Learned: Openness & Respect for Others, Social Responsibility |
| It was a mixture of nervousness and pride [to have people look at my work]. On one hand I didn’t know if my idea would be communicated thoroughly, but then I realized that it was okay if someone didn’t see my exact thought process. Their interpretation could have been different and just as good, if not better! *P9 |
| I think the community learned that PT is so much more than exercise. I think one of the eye opening things about the art show was that the underlying theme for the majority of the work was community. So many pictures detailed a multitude of people working together. *P3 |
| What I learned about myself through this process that it is important to be open to all types of learning. Although this is something that I [have] rarely done, it allowed for me to access another part of my brain that is rarely used in PT school and that I haven’t used for some time but it was something that I used to do very frequently. I think that I will start implementing the use of more artistic ways to study because I believe that it is very beneficial. *P20 |
| Calling to Physical Therapy Confirmed as Vocation |
| I learned that I have chosen the right profession for me. Through the creation of my artwork l was able to reflect on what physical therapy means to me and how I am able to use the skills that I have learned to educate others in the community and to help improve each patient’s quality of life. l was able to reflect and understand the great gift that physical therapy is able to offer to those in the profession and those in the community. *P3 |
| I learned how creative and talented everyone is in our class. There were some amazing drawings, painting, sculpture, colleagues, and 3-D art. It was incredible to see how much work everyone put into the project. It was neat to see how everyone sees physical therapy differently and how each of our experiences truly shape what we believe in. We are all called to this profession and how we answer our call to practice can be expressed in art. *P31 |
| I learned that I should engage in more creative activities because I do have some talent and good ideas. I learned I should just trust an experience to take me where I need to be and just because I don’t understand the purpose at the beginning doesn’t mean I won’t at the end. I also learned that I have a very strong view of physical therapy and what it means to me. *P37 |
*P# = Participant number
Third-year students in the program were asked to create a piece of art for an art show being staged to celebrate Physical Therapy Month in October as part of a Critical Integration DPT course in the last year of the curriculum in a Midwestern university. The theme of the art project explored the intersection of the World Health Organization (WHO) ICF Model30 and the new vision statement for the American Physical Therapy Association (APTA) which states physical therapy has a role in “Transforming society by optimizing movement to improve the human experience.”20,21 The ICF model moves beyond a medical diagnosis and utilizes a more holistic approach to examine a person’s participation in societal roles despite potential medical diagnosis, functional and activity limitations, as well as environmental and personal contexts which either promote or limit participation in life roles. Students created paintings, sculptures, poems, photographs, flipbooks, collages, or other works of art to express intersection between the ICF Model and the APTA Vision Statement.
Several reflective journals were made available for community member guests to record their thoughts while attending the art show. These handwritten reflections were transcribed for analysis. No names were attached to journal reflections of the community members. The reflective papers from students and transcribed comments from the community were analyzed for themes and a common description of the experience was created. Forty responses were provided from the student artist group and 30 were obtained from community participants. See Figure 1 for the research process used in this study.

Data Analysis
The reflective papers from the student artists and the written community reflections were analyzed using a descriptive phenomenological approach described by Giorgi27,28 and Dahlberg, Drew, and Nyström.26 This process involved a whole-parts-whole-type holistic examination of the interview texts until constituents or themes of the experience were revealed. Each reflection by the student artists was read two times with the intent to become familiar with the overall tone, word choices, and phrasing. The third reading attended to the flow and structure of the text created by the student artists and main segments of the community participants’ writings were outlined. On the fourth and final reading, key descriptive words or phrases were identified. Important phrases and lists of common elements were used to create a summary of the experience for each participant. Identities of the reflective paper authors were confidential to the primary investigator but anonymous to the other researchers on the team.
The research team collaborated to summarize the essence of the experience with the themes generated by this process. The researchers created a narrative summary and a thematic summary for each participant. These themes were emailed to the student artists who were asked if the interpretation matched the way they lived the art show experience and if the researchers misunderstood or misrepresented anything in the interpretation. Without the participants’ ultimate approval, any descriptions or interpretations of the research team would be inadequate and possibly biased. This process served as a vertical analysis for each reflection received from the student artists. A similar process for completed for the community member reflections. Since the authors of the community writings were anonymous, the common narrative summary and themes were shared with community members who attended the art show after the opening night, but who did not provide reflective writings.
Finally, a horizontal analysis across all written reflections was completed to develop the common description of the experience of staging an art show by the DPT students. Once this process was completed, a summary of the common description and themes across all reflective writings by student artists were shared with the students for review to determine whether or not the common description resonated with the experiences of the student participants. This process also helped ensure dependability and credibility across all student reflections through the member checking process of the common themes. A similar process was used to analyze reflective descriptions of the community members attending the art show. This common description summary was shared with community members who were not a part of this study and did not attend the art show. Saturation was reached by community members after receiving comments from 10 individuals. This process was done to solidify credibility and trustworthiness of the description for the community experience.
Methodological Rigor
Methodological rigor is as important in phenomenology as in other forms of qualitative or quantitative research. Thomas et al24 suggest that the aim of phenomenological research is to find meaning and understanding as opposed to causality and prediction; the criteria to evaluate the rigor of phenomenology is slightly different than what is used in a positivistic process of research. In this case, phenomenological research answers the research questions and the description of the lived experience provides fidelity to the knowledge claim about a lived experience.31 A relationship is thus established between researchers and the community to which the knowledge claim is presented. Furthermore, McClelland states the job of the researcher is to “seek an authentic telling of the experiences and what they mean from the perspective of the participant.”32(p. 178) In this study, methodological rigor was established by allowing participants to engage in the data analysis process by providing clarifying comments about their own descriptions and the common description formed by the analysis across all participants. Hence, CBPR and phenomenology were used to provide a rich description of the elements of everyday life or lived experiences of those being studied to describe how the visual art experience helped student artists and community members better understand the role of physical therapy in society.
Results
Themes and comments from the student artists are listed in Table 3. Students reported being skeptical about the art show initially, but eventually obtaining a deeper understanding of how they may transform society and improve patient care through this assignment. Although the experience was challenging for most students, it helped them confirm that they had chosen the right profession. All students reported being challenged in new ways and they were proud of their use of art to communicate and promote the physical therapy profession. Finally, all students had a plan for displaying their art after the show and ideas regarding an expanded role of advocacy and community engagement.
 |  |
 |  |
 | |
Figures 2 – 6 show examples of the visual art created by the student artists. Student reflections on the project illustrate the lessons that were learned:
Now after completing the art show, I understand that we can use different types of media in order to convey what physical therapy is to the community as a form of education. I also feel that in many ways when we treat patients we have to act as artists and be creative in the way that we work with our patients and the unique interventions that we implement for each unique patient to improve their function and engagement in life. *P3
Another student reflected on lessons learned by engaging the community through an art show and the future role in society as a professional:
I am now able to see more clearly how to engage the community about issues I am passionate about regarding my profession of physical therapy and advocating for my patients. How can I NOT have a voice about something I feel is so important for society and the health of my patients? *P24
Common themes also arose from the writings of the community members who attended the art show. The community reported gaining a better understanding of physical therapy as a profession and the role played by the profession in the community. Community members described PTs as healers and educators who solve complex movement problems and bring hope to those with movement disorders. Physical therapists were seen as medical professionals who specialize in movement by community members. Additionally, community members in attendance at the art show stated they would feel comfortable discussing personal movement and health problems with a PT after attending the art show. Community members reported feeling a deep connection to the physical therapy profession through the art and shared personal stories of encounters with the physical therapy professionals in the journals. See Table 4 for comments from the community members.
Table 4: Themes and Comments from Community Members at the Art Show
| Physical Therapists as Movement Healers |
| I learned a great deal from the art show about Physical Therapy. I had no idea that PTs did so much to help people of all ages move better. There are so many settings that PTs work in. They are extremely talented and creative. I will consider seeing a PT first the next time I have pain that needs to be healed. Now I know there is hope for me. *CME #2 |
| Physical therapists are movement artists who use the human body as their creative canvas. Their eyes are assessment tools. Their hands are the implements of healing and their minds hold the genius ability to connect movement science from book learning to a recipe for success and better movement in real life. PTs heal people of all ages with movement problems. They are also pretty decent artists as well. *CME #23 |
| The art show brought tears to my eyes. I was speechless! It was wonderful. I had no idea how many different things physical therapists do to improve human lives. I was impressed at how talented the students are. They are gifted scholar artists who also use their talents to heal people with movement afflictions. They do more than improve function. They improve quality of life. *CME #28 |
| Physical Therapists as Educators & Artists |
| I especially loved the interactive nature of this art show exploring movement in a person’s environment. I learned so much today about physical therapy. The students were so creative and their work was as excellent as anything I have seen from an art student or art school programs. Today I learned how art skills translate into learning about the body and helping people recover from devastating illness that limits movement. I feel I learned a lot today. I am inspired. *CME #8 |
| The art in this show spoke to my soul. It was all so different and yet so much the same – dealing with how PTs bring hope to people who are suffering from movement problems. I learned there are so many things I could go talk to a PT about. I would feel very comfortable sharing my movement problems with a PT. They will have good insight on my situation, my space in the office and my world. They will teach me to prevent ongoing problems. *CME #14 |
| Physical Therapists can help teach us how to move better. With so many body types that is a challenge but I now know PTs are up to the task. These students were remarkable. I learned so much about the message behind the art from the student artists as well. Now I know what kind of work PTs do. The art taught me so much on so many levels. *CME #19 |
| Connection to the Profession |
| I would definitely go see a PT after experiencing this art show. I learned that we will all have our troubles and lose hope some days. It is nice to know what professional to choose if I am having a problem with my movement. I know I could talk to a PT now. I don’t have to just go to the doctor or a nurse for help. That gives me hope to know that someone will take time to work with me to move better and improve my life. I now know I can ask my physician for PT. *CME #6 |
| I was amazed at what these students and faculty were able to do in the world of art here at the gallery. I believe that if my quality of life is affected by a movement problem, a PT is who to go see to solve my problems. They know so much! I would be very comfortable talking to a PT about my problems. I now have hope about my chronic movement problems. I will ask for a referral to PT from the MD. *CME #12 |
| I feel a strong connection to the profession. PT is not just about muscles, bones, and nerves. There is a great deal that PTs do to bring hope and improve function. They play a role in making a patient’s quality of life better. There is a lot they have to offer us and I think everyone needs to have their own personal “PT guy” of “PT gal” like people have their own doctor or financial planner. *CME #27 |
*CME#: Community Member Exemplar Number
Discussion
This study used a sample of DPT students (n= 40) and community members (n= 30) to qualitatively explore the experiences of DPT students who created an art project for an art show on a Midwestern university campus. It also explored experiences of community members who attended the art show through reflective writing about the experience. The reflective writings of the DPT students and community members revealed a greater understanding of physical therapy as a profession or calling. Students learned about the participatory nature their work inspired among themselves and the greater community in attendance at the art show. Lessons about the profession of physical therapy were learned by all stakeholders.
From the student perspective, there was a degree of initial skepticism regarding the assignment, followed by anxiety about what type of art to create for the art show. As students were provided with time and a safe space, levels of anxiety diminished and were reframed as excitement and anticipation for the show. The art assignment was viewed as a challenging but rewarding task. In their work with occupational and physiotherapy students, Smith et al15 reported student reactions to incorporating arts into the curriculum was initially met with anxiety because many therapy students had little time to do any artistic work prior to the arts assignment. Rabow 14 reported similar findings in the study on art and physicians. Students in our study were no different, with many experiencing an initial level of anxiety toward the assignment and finding it a challenge to incorporate art into the capstone coursework despite having adequate time to prepare. Students stated they eventually found the assignment to be relaxing and creating an art project provided a release for anxiety. Middleton and Drucquer11 reported similar findings and emphasized the importance of medical professionals utilizing art as a method to mitigate the everyday stress and demands of professional life.
Students in this study thought a great deal about the assignment, engaged in self-reflection on the task, and took great ownership of their work. When staging the art show, there was an interesting transition of thought as students began to mount their art. Students were initially nervous about others’ opinions of their work. Once fully staged, the students took a step back to examine the art in the show before the opening night. Student reported taking great pride in their work. Once staged, the private art work became a public extension of the embodied self. Merleau-Ponty33 described the thinly veiled line between subject-object relationship in his writings. Other authors in health care education describe how artistic expression encourages students to view patients more holistically, making an emotional connection to issues in health care, and taking a stand on an issue.6,14,15 Although, initially uncomfortable, this connection to the humanity of others leads to deeper practitioner self-reflection with less judgmental attitudes and an increased openness to new ideas.7,9,14,15,16,18 The DPT student artists in this study expressed an openness to classmates’ work and a renewed realization that physical therapy was a calling to vocation which concurs with Smith et al15 and Whitham et al.16
A local newspaper announcement and university communications advertised the art show. The community in attendance had an opportunity to talk with the DPT student artists about their work. Many stories were shared about physical therapy experiences. These stories diminished the distance between the DPT students and those who had suffered movement restrictions that limited full participation in life roles. Social issues regarding experiences with disability, insurance coverage, and the role of physical therapy in addressing social problems were brought into a public space. The DPT students and community members were able to discuss the biopsychosocial nature of the barriers to health and wellness that individuals face in the community. Stories and lessons regarding access to physical therapy care were exchanged between students and community members. The use of CBPR has been used to raise awareness of health and well-being in a community with the ultimate purpose to eliminate health disparities.29 HH have been demonstrated to connect medical and allied healthcare students to connect with and engage social problems in their lives.7,9,13-16,18,19 At the art show, potential solutions to health disparity were discussed in the context of social responsibility and awareness was raised about the opportunities of PTs to enhance the health and wellness of the community.
A calling to the profession of physical therapy was identified and reaffirmed by students through the experience of participating in the art show. Students in this study felt the art show provided a portal for transition from student to entry-level clinician and a new way to communicate with others. Students reported previously losing the vision for why they enrolled in a DPT professional curriculum.6,15 Evans reported MH and stories of everyday experiences allow professionals to connect to patients on an embodied level, find connections to social problems, and reflect on their role in society as a professional.6 Smith et al15 echo the importance of MH in allowing students to reflect and verify a calling to a chosen profession. Students in this study reported a deepening of their understanding of the role of social responsibility and community engagement as part of one’s calling to a profession and a renewed confidence in their choice of vocation.
Mission and vision statements of organizations provide lofty goals for transcending silos. The profession of physical therapy has been working to educate its own members and the community about physical therapy and what physical therapists do as professionals. Finding a connection between the profession of physical therapy, the world of academia, and the community is a challenge. Yet, HH appears to dismantle boundaries of the silos segregating professions and academia from the community. The incorporation of HH in educational programs may provide a means to better understand community needs and educate the community on the profession of physical therapy by illustrating the potential of physical therapy to transform society by enhancing movement to improve the human experience.
Strengths and Limitations
Strengths of the study include a relatively large sample of reflections from DPT students (n=40) and community members (n=30) ensuring a variety of descriptions were obtained. Resonance around member comments reached saturation after 10 reviews of the common description for the art show. The investigators were experienced at conducting phenomenological research.
A few limitations exist. The researchers acknowledge the results of this study may not apply to all DPT programs or communities. Staging an art show may not yield similar responses from students or the community whether it is done earlier or in the later stages in the DPT curriculum. Visual art is such a personal and public medium of expression. Meanings constructed from the art may vary depending on lived experiences of those creating and those viewing the art. A sense of reciprocity exists as a result of the experience.
Future Study Recommendations
Researchers may consider investigating how HH influences observations skills of physical therapists and physical therapist assistants. Claims have been made that HH improves clinical observation skills allowing physicians, nurses, and occupational therapists to develop better differential diagnosis skills and holistic treatments skills.8,12,14,15 No such study has been conducted among physical therapists. With some form of direct access in all 50 U.S. states, it will be crucial for physical therapists to hone observation skills to be able to identify patterns of symptoms that require referral to other healthcare providers for optimal patient care.
Conclusion
The visual arts and HH provide opportunities for deep connections to new ways of thinking about the human condition in physical therapy education and in society. The community learned about and gained new appreciation of the work of physical therapists through the experience of attending an art show. Students and community members were inspired and surprised by the power of visual art to explain the profession of physical therapy and the ways physical therapists can improve the human experience. Through the art show experience, students learned new ways to problem solve and consider alternative methods of expressing the essence of their personal beliefs about physical therapy and professional roles in transforming society. Through experiential education of an art show, the community learned about the profession of physical therapy and the role it may play in their lives when facing the distress of activity limitations preventing full participation in life roles. Community members learned strategies for advocating for their health needs by asking for PT referrals from their physicians if not provided. It appeared that a patient-therapist connection between the community and the profession was created. True service and the elimination of need cannot occur unless knowledge about a profession and society is made available in a translational manner. Ultimately, better serving our patients through the establishment of a deeper understanding of the patient-practitioner relationships is how the human condition is enhanced and society transformed.




In the late 1990s, a patient was referred to my Neuropsychiatry clinic. She was a middle-aged woman who had been brought to the Emergency Room by ambulance with signs and symptoms initially suggestive of a stroke. However, brain imaging was normal and neurological examination revealed certain, atypical signs that suggested a primary psychiatric disturbance (sensory changes that did not fit a dermatomal distribution, a level of consciousness that waxed and waned). The diagnosis of conversion disorder was made, correctly, as subsequent events revealed.
By the time she arrived to see me, the quasi-neurological difficulties were resolving. She was now able to give a full and eloquent history. I learnt that she was a front-line journalist who had recently returned from covering a famine in East Africa. This was not her first exposure to frontline journalism–her career stretched back over a decade – but it was amongst her most traumatic assignments for she had witnessed mass starvation and death on an enormous scale. Distressed by what she was witnessing, she had resorted to alcohol as a way of damping her anxiety and helping her fall asleep. She managed to limp through her period in the field, keeping her emotions under control. On returning to Toronto, she thought she had put the worst behind her. It was while sitting in a restaurant with her husband that she suddenly found it difficult to speak and stay awake. Her husband, understandably alarmed, had called the ambulance.

One of the aspects of her history that intrigued me was her initial reluctance to acknowledge her emotional distress and reach out for help. She was aware, while out in the field, that her moods were awry and that she was becoming increasingly anxious. And yet she had done nothing about this, other than resort to alcohol to self-medicate her distress. She worked for a large, well-resourced news organization–why had she not contacted someone for help? Her answer gave me an immediate insight into the world of the foreign correspondent, cutting through my naiveté and revealing one of the hidden challenges faced by these most public of journalists. “You don’t understand my profession,” she told me. “If you let on that you are emotionally unwell, you will never again be sent on these types of assignments. It means the end of your career. You muddle through, but you never let on how you are feeling. We all know this.”

Taken aback by this revelation, and frankly skeptical of her assertions, I asked my research team to take a few hours off from their brain imaging work which focused on depression in people with multiple sclerosis, and to search the literature to see what had been written on the subject of war, conflict, and the psychological wellbeing of journalists. A second surprise was in store for me. Not a single article appeared in the Medline and PsycINFO databases. Behavioral researchers had passed it by. Notwithstanding a formidable amount of research devoted to psychological trauma in veterans, fire-fighters, police officers, and victims of assault and rape, amongst others, no research had been devoted to journalists who covered war and disasters. There would be no insights forthcoming from the medical and psychological literature.
I was intrigued as much by the absence of any research on the subject as by my patient’s presentation. She was a fascinating person to treat for she had traveled the world for a decade, bringing back news of far-flung conflicts for a Canadian public keen to be kept informed. Unbeknownst to her readers, and until recently her psychiatrist, was the emotional toll this work had taken on her.

“Chance favours the prepared mind,” observed Louis Pasteur. My long-standing interest in psychological trauma left me curious to know more about the psychological wellbeing of war and conflict journalists. My patient’s interesting career, which had afforded her a ringside seat as history unfolded, spurred me to write a grant application and submit it to the Freedom Forum in Washington, D.C. I proposed a detailed study, looking at rates of psychopathology in war journalists. The grant was funded, a collaboration was forged with John Owen, Director of the Freedom Forum’s office in London, and the results of the 18-month study were published in the American Journal of Psychiatry on the one year anniversary of the attacks of September 11.1 Major news organizations (CNN, BBC, Reuters, the Associated Press) had been keen to take part and had opened their roster of correspondents to me. The 140 journalists who took part were no less eager to tell me how they were feeling. The data revealed a high lifetime prevalence of posttraumatic stress disorder (PTSD) and major depression, with rates of the former approaching that seen in combat veterans. Here the emphasis on lifetime is important because my research underscored both the cumulative nature of the risks confronted and, by extension, the accumulating burden of psychiatric illness. For one of the most remarkable statistics to emerge from this study was the longevity of exposure to grave danger that is integral to war reporting. On average, the journalists had spent 15 years working in war zones; a remarkable statistic, and a duration of exposure to potentially life-threatening events that is surely unrivalled by any other profession, the military included. And this for a profession not schooled in violence.

To the credit of the news organizations taking part in the study, the one statistic that they found of even greater interest and importance was the one that showed very clearly that journalists with PTSD and depression were no more likely to be receiving psychiatric treatment than their colleagues who did not have these disorders. This finding has led to a sea change in attitudes amongst many of the media organizations in North American and Europe that send journalists into harm’s way. They now recognize that it is insufficient to focus on physical safety alone. War, disaster, and conflict may leave a journalist physically unscathed, but psychologically scarred. Here were data attesting to this and moreover, these data carried implications that extended beyond the immediate health of the journalists. PTSD and depression can affect the wellbeing of family, friends, and colleagues as well. To news organizations maintaining bureaus in countries that had become war zones, like Iraq and Afghanistan, having a journalist with PTSD on site could compromise the safety of colleagues. A traumatized journalist can behave erratically, display impaired judgment, show increased irritability and, in general, undermine the safety and cohesiveness of a bureau already under siege in a hostile locale. Therefore, it is imperative for those in need to receive the requisite therapy. Effective treatments, be it cognitive-behavior therapy, prolonged exposure therapy, or Eye Movement Desensitization and Reprocessing, are all available within a Western health care system.

This initial study raised more questions than answers. Subsequent studies each addressed a different question: how were domestic journalists in New York City faring psychologically after 9/11?2 Was it psychologically helpful or harmful for journalists to be embedded with the military during the Iraq War?3 Could one predict, based on cognitive constructs, which journalism students would chose the foreign correspondent career track?4
Another avenue of research pursued was to investigate the emotional health of local journalists working in dangerous places. UNESCO commissioned a study of Mexican journalists.5 Studies of Kenyan6 and Iranian7 journalists were also subsequently completed. Notwithstanding the disparate cultural backgrounds of these journalists, a consistent finding emerged. PTSD, depression, and substance abuse were significantly more likely to occur in journalists who had been traumatized. However, unlike in my earlier study which prompted Western news organizations to become more responsive to the emotional health of their journalists and make therapy available to them, no such change occurred outside Canada, the USA, and Europe. Non-western journalists covering news of war, revolution, and corruption are threatened, assaulted, kidnapped, tortured and killed and little or no help is offered to those who survive. For some, the psychological consequences of these stressors are profoundly disabling.
All war journalists are exposed to grave danger, but the degree of exposure is highest amongst the photojournalists. This is inevitable given the nature of their work. You cannot hang back from the fray and get a good photograph. The risks, high to begin with, increase with close proximity to the event. This observation led me to explore, in greater depth, the lives and careers of 12 extraordinary war conflict photographers. The project was supported by the Globe and Mail, Canada’s national newspaper and the series may be found at http://tgam.ca/ShootingWar.

I chose photojournalists based on my familiarity with their work. My idea was to select one photograph from the portfolio of each photographer. Each photograph, for a variety of reasons, told a powerful story. The series reveals not only the extraordinary creativity of the photographers and the dangers that they confront in pursuing their work, but also the costs paid in doing so. When you go behind the lens and explore the lives of these contemporary visual historians, it becomes readily apparent that bravery and creativity, while necessary prerequisites for this kind of work, are no antidote to physical, emotional and moral injury. Although I am concentrating on Joao Silva’s image and story for this article, I offer the briefest of summaries of the costs paid by the other eleven photojournalists: Ron Haviv marked for assassination by a rogue warlord, David (Chim) Seymour killed at Suez, Corinne Dufka blown up in her armoured vehicle and wounded, Santiago Lyon wounded, Don McCullin wounded multiple times, Tim Page wounded five times in Vietnam (including a penetrating traumatic brain injury), Sebastiao Salgado incapacitated by physical and emotional exhaustion, Ashley Gilbertson brought down by guilt, Alexandra Boulat deceased at 45 years of age (albeit not combat-related), and Robin Hammond incarcerated and intimidated by Robert Mugabe’s goons. Faced with this array of life-threatening stressors, it should not come as a surprise that, for some of these photojournalists, post-traumatic stress disorder has added considerably to the challenges faced. The only photographer untouched by a malevolent hand was the amateur amongst them, banker Charles Porter, a man who never visited war zones, but who happened to have his camera with him in his Oklahoma City office on April 19, 1995, the day Timothy McVeigh blew up the Alfred P. Murrah Federal Building. Porter, who subsequently left his banking job and became a physical therapist, is the only one amongst this pantheon of photojournalist greats to win a Pulitzer for his work, lending credence to Susan Sontag’s opinion that:
Photography is the only major art in which professional training and years of experience do not confer an insuperable advantage over the untrained and inexperienced – this for many reasons, among them the large role that chance (or luck) plays in the taking of pictures, and the bias towards the spontaneous, the rough, the imperfect. (There is no comparable level playing field in literature . . .or in the performing arts . . . or in film-making. . .) 8
By design, I began my series with Joao Silva. On October 23, 2010, while on patrol with American marines in Afghanistan as an embedded photographer for the New York Times, he stepped on a landmine. Fifty six years earlier, the legendary photojournalist Robert Capa had done the same thing in Vietnam. Capa died, Silva did not, his survival due to the extraordinary progress made by military medicine in the intervening years. Silva’s injuries were grievous. His legs were shredded and he had extensive abdominal trauma. Thrown to the ground by the force of the blast, lying in the dust of Afghanistan, conscious and cognizant of his life threatening injuries, Silva’s first impulse was to continue taking photographs. He gets off three frames before the medics take his camera away from him and begin saving his life.
 |  |  |
His insouciance in the face of death, his composure in reaching for his camera to take photographs, his relentless drive to keep working in the face of his own potentially imminent death – these were some of the factors that made me want to begin my series with Joao’s remarkable photographs. Silva was no neophyte when he stepped on that landmine. His pedigree as a conflict photographer went back to 1994, when he covered the run-up to the first multiracial democratic election in South Africa, a particularly violent time in which he witnessed and photographed the death of his close friend and fellow-photojournalist, Ken Oosterbrook.

I had interviewed Silva twice before he was injured in Afghanistan, both times in his home city of Johannesburg, South Africa and with the photographer in robust health. When we met again, post-Afghanistan, the circumstances were very different. He was living alone in an apartment in Bethesda, provided for him by the New York Times so that he could be close to his medical team at the Walter Reed National Military Medical Centre. His in-patient care was over, but extensive rehabilitation was still needed. Not only had Silva undergone a bilateral leg amputation, he had been left with a persistence abdominal wall infection that required weekly surgical interventions under general anesthetic. His life, far from his wife and young children, had been given over to a succession of medical appointments and interventions. He was in constant pain. His diet was severely curtailed. Ambulation on his prostheses was challenging. It remained unclear whether he would be able to work as a photojournalist again. A mountain of obstacles lay ahead, but his spirit had not been broken. The fortitude he had brought to his work as a war photographer, the courage that he had shown in photographing the burning township in South Africa and the Mahdi’s army during the war in Iraq, was now self-directed and being applied to his own rehabilitation.
This is not to say Silva’s mood was upbeat. As he described it to me, he had been in a very dark place during his hospital stay and he was not out of the woods yet. But he coped by keeping his focus, harnessing an enormous willpower, taking one day at a time, staying in the here and now, keeping his attention and energies on the tasks that each hour brought, and refusing to allow his thoughts about an uncertain future to run away with him. His resilience was astounding. There were no signs of PTSD. The doctors at Bethesda were impressed by his fortitude. The psychiatrists went with their students to interview him, to learn from him and to try and understand what it was about this man that allowed him to marshal his coping resources so effectively.
I was no less intrigued. Listening to Joao speak about his recovery, from the earliest days in a military hospital in Germany to his stay in Bethesda, I became aware of what a long, hard, and lonely road he had traveled, in spite of the excellent care he received. His rehabilitation was as much about his own inner journey as it was about the surgeries undergone and the prostheses fitted. It was clear to me that he had never once entertained the thought of failure. There was only one option open to him and that was recovery. In those wee small hours of the morning, where there is no place to hide from one’s fears, when the thought of defeat, of not being able to surmount a myriad of medical problems, was most likely to surface, he fought his demons and beat them. I can only imagine how hard this must have been for him, and imagination surely falls short in circumstances like these. With each setback, and there were many, he would pick himself up and start all over again, his steely resolve fixed on being able to walk unassisted, his body free of infection. No one taught him this. From the moment he fell, reaching for his camera to record the moment, to those long days and even longer nights in a lonely Bethesda bedroom community, an innate resilience was evident. I have no doubt that this behavioral trait was integral to his ultimately successful rehabilitation. When we met again, a year later in Johannesburg, Joao was on assignment once more for the New York Times. His war days may have been over, but a subsequent email sent from Paris made me smile – he was back on the road, en route to Togo.
The drive and determination that Joao Silva displayed as a war journalist, the very traits that allowed him to gain access to the world’s most dangerous places, stood him in good stead during his rehabilitation. None of the other 11 journalists I interviewed for my “Shooting War” series, apart from Tim Page, suffered physically to the same degree. But all had voluntarily journeyed into the vortex of conflict to do their work, each drawing on a deep well of courage and fierce desire to record history with a camera. These attributes of temperament not only allow them to fulfill an important civic function, namely keeping societies informed of world events that in an age of globalization affect us all, but also to overcome the fall-out that comes from working in zones of conflict. Here no distinction is made between the physical and emotional, for as Joao Silva’s history so clearly reveals, both are tightly intertwined. The fact that health care specialists who work in rehabilitation have long known this does not diminish the lessons to be learned from the careers and tribulations of the great war photographers. Affirmation too can prove inspiring. Overcoming the odds, at times insuperable, is a theme that readily resonates within the rehabilitation community, for patients and therapists alike. It is no stranger to the war photographers too. With thanks to Moe Doiron, Photo Editor at the Globe and Mail, and Joao Silva.
All requests for copies, distribution or derivatives should be made directly to the author.


This work is licensed under a Creative Commons Attribution 4.0 International License.
 In 2009, Bill Forester became one of the 790,000 people in the United States to suffer a debilitating stroke. He was also a part of the two thirds of this group that required rehabilitation services1 to recover some of their previous independence. A stroke survivor’s experience with rehabilitation is undoubtedly affected by their ability to cope with the sudden change to their life plans, expectations, and self-identities. Bill Forester’s experience of rehabilitation, and his discovery of latent artistic talents, clearly highlights the ability of the human brain to adapt following a stroke. His story also reveals the capacity of the human spirit to grow through nurturing relationships with family, therapists, and even accidental friends. Bill discovered his unique potential for rehabilitation through the guidance of those around him, but it was his unyielding motivation to recover what he had lost that allowed him to discover a part of himself that he had never suspected.
In 2009, Bill Forester became one of the 790,000 people in the United States to suffer a debilitating stroke. He was also a part of the two thirds of this group that required rehabilitation services1 to recover some of their previous independence. A stroke survivor’s experience with rehabilitation is undoubtedly affected by their ability to cope with the sudden change to their life plans, expectations, and self-identities. Bill Forester’s experience of rehabilitation, and his discovery of latent artistic talents, clearly highlights the ability of the human brain to adapt following a stroke. His story also reveals the capacity of the human spirit to grow through nurturing relationships with family, therapists, and even accidental friends. Bill discovered his unique potential for rehabilitation through the guidance of those around him, but it was his unyielding motivation to recover what he had lost that allowed him to discover a part of himself that he had never suspected.
Prior to his stroke, Bill had worked as a professor, a public speaker, and a realtor. When confronted with the reality that he could not return to work following his stroke, Bill and his family devoted their time and energy to his rehabilitation. What resulted from their efforts are an ambitious story of trial and error and the discovery of painting as a medium for rehabilitation.
Art became a critical component of Bill’s rehabilitation and an essential aspect of his new self-identify. Today, you can find Bill at his friend’s art studio in Cleveland, Ohio. He will mostly likely be working on a commissioned landscape or portrait painting. Or he may be preparing for his next speaking engagement at a local hospital or university, where he motivates rehabilitation therapists and stroke patients to push each other throughout the recovery process. He uses these opportunities to explain that it was the love and devotion of his therapists and his family that re-instilled in him a sense of self-worth and that continues to drive him to reach his full potential as an artist, a husband, and as a friend. Wherever you find him, you can be sure that he will be cracking jokes and enjoying every minute that life has given him.
Video: Art Saved My Life
In “Art Saved My Life,” Bill describes how he discovered painting as a unique form of rehabilitation after suffering a debilitating stroke in 2009.
“When I was painting, I saw myself being an artist… and I had a sense of being again.”
Video: Accidental Friends
In “Accidental Friends,” Bill describes how the love of his family and therapists motivated him through the long rehabilitation process after his stroke.
“People will ask me what is my secret to recovery… it’s love!”
The Right Hand of StrokeI am Bill’s right hand. Together we learned how to color, how to draw, and eventually how to write. We learned from every “nick” that we got while we shaved, and we blushed as we held the hand of our very first girlfriend. Together we shared all of the hard times, all of the fantastic memories, and all of the inappropriate stories that one might expect from a life as full and as active as ours was. We cradled our baby children and we comforted our wife. Throughout our career as a public speaker, realtor, and college professor, we worked in unison. It never occurred to us that this connection, that had always been so effortless, could be broken. It wasn’t until our connection was abruptly interrupted on April 17, 2009 that we were able to appreciate what we had lost. Bill says he died that day. This was the date that marked the beginning of our journey to re-establish our bond, which had been so important to who we were. The last thing that I was able to do for us before our connection was interrupted was to signal for help when Bill lost his balance, could not see straight, and when his voice failed him that fateful day seven years ago. We knew that his daughter was in the house, and she would help if we could get her attention. We managed to knock everything off of the bedroom dresser, creating a huge racket, before we crumpled in a heap to the floor. I could sense Bill trying to get me to do more, but I was unable to respond, There was nothing more that I, Bill’s trusty right hand, could do, in our hour of need. With his daughter alerted, a new fear sprung to mind and shot down to the tips of our fingers. I felt Bill summon everything he could muster to crawl, one hand, one leg, to block the door. “I don’t want my daughter to see me die,” I could still sense Bill’s frantic thoughts. When we heard her say that she had called her brother, everything calmed. “That was my purpose. Get someone else to help her, to be with her” Bill thought. When the paramedics arrived, we heard everything: sirens, commotion, frenzied voices telling Bill to relax. This was strange since in our mind, we were completely calm. However, the scars from the restraints they had to use to get us to the hospital tell a different story. We did not let go of our bond so easily, this precious connection between mind and body. But neither him nor I were in control. And so we resisted the paramedics all the way to the hospital, without either of us knowing it. When we arrived to the community hospital, we could hear all of the doctors, technicians, and nurses. We heard when the doctors encouraged his wife to accompany us on the “life flight” to a larger hospital in the city. They didn’t think Bill would survive the trip. Before we found out what had actually happened–that we had suffered a massive hemorrhagic stroke on the left side of our brain–Bill remembers seeing his wife crying. He saw the anguish quickly spread across her face, and to this day he will tell you that one of the hardest things about having a stroke was seeing his family’s grief. He kept trying to tell them that everything would be ok, but he could not. He could not speak. He wanted me to reach out to them, to comfort them. But I could not. So I stayed there, lying limp by his side. Bill was upset that he could not control his muscles like he used to, but he was most upset he could not speak. When one of the doctors asked his wife if Bill had a living will for organ donation, Bill tried to scream out to him: “I am still using my organs! I need all of my organs right where there are!” But nothing came out, and no one heard him. Then the doctor asked his wife about Do Not Resuscitate orders. “Yes! Please! Resuscitate me!” Bill begged them silently. His wife consulted his children. I sensed the fear and confusion that Bill felt, and it was startling. Not only did we not know what was going to happen to us, we could not even tell the people we loved most that we were still present, we were not lost yet. Bill decided while we were still in the hospital that we would find a way back to his family, to himself, and to his life. We felt our first sense of relief upon leaving the hospital, and meeting our Occupational Therapist, Cindy Clark. In addition to the support of Bill’s wife and family, Cindy was part of a group of dedicated rehabilitation professionals that would guide us our on journey, and help us reclaim our connection with each other. They would help us relearn everything that the stroke had erased. When we met Cindy, we were eager to get to work. Work is what we were good at after all, before the stroke. When Bill could not get me reach out to Cindy for help, she took us in her own hands and showed us step by step, how to do the things that we had forgotten. It was slow, clumsy work at first. We had no sensation at all from our shoulder down to our fingertips on the right side. Fine motor skills, which once had come so naturally, now became painstaking work. As far as I could tell, Bill had forgotten about our right side all together. We would frequently bump our right shoulder and arm into walls and cabinets; unaware of the bruises this would cause. Cindy helped bring Bill’s attention back to his right side and to his right hand. And slowly, I began to respond, at least somewhat, to what Bill wanted to do. We did everything the therapists wanted us to do in the clinic. Once we had exhausted the typical exercises, we wanted more. So Cindy signed us up to participate in a community run. We thought this was strange since Bill had never really run before the stroke. He seemed to enjoy it however, as we began training for a marathon after we completed that first race. Then Cindy told Bill that she wanted us to throw out the opening pitch at a local baseball game. Though we both thought that she was crazy, we practiced. And practiced. And every day that we practiced we could feel our connection grow a little stronger. Cindy taught us, hand over hand, how to hold the ball and when to let it go. Eventually we re-mastered the sequence. I was surprised that when the time came, as we stood alone on the pitcher’s mound, we did not feel fear, but pride, for having made it this far. Somehow we managed to let the ball loose, just as we had learned. I was with Bill as he enlisted the help of teachers and voice coaches, and as he began to seek out other activities that might help us rediscover our sense of self. It took one whole year before Bill was able to speak again, and then aphasia made getting his words out challenging. We decided to spend six months with an artist friend in San Pedro, Mexico. Two days a week, we taught English to locals. This is how Bill began to reclaim his words.
While we were in Mexico, we started painting. Bill forced me to do the work, which was new to both of us. He forced me to hold the brush and to follow the lines that he set out. I squeezed cyan, magenta, whites and blacks out of their tiny tin tubes and mixed color after color on the pallet. He did not let me rest by his side, though it would have been much easier for us. When we got back to Cleveland, Bill bought an easel and befriended a local artist who began teaching us about painting. And then painting became our routine. It became our motivation and stress relief. It was something to look forward to, and something that showed us how far we had come.
While painting, something strange happened. We would start with the darkest darks and the lightest whites. In bringing together these extremes, Bill began to find himself on the canvas. Through self-portrait after self-portrait, an image of being became clear to us both. We were artists now. Life was simple now. This activity, which seemed so superfluous to Bill before the stroke, allowed us to continue to work on regaining strength, coordination, and control of our muscles. It made it easier for Bill to formulate his words and speak his mind. Bill reached into himself to recover. In delineating his profile on the canvas, he allowed his true self, his NEW self, to come into being. Now we are working again. We have been commissioned for landscapes and portraits from customers who really like our work. I wonder though, every time someone likes our paintings or asks to purchase one, if they realize the journey that we–Bill and his right hand–went through to get to where we are now. The paint on the canvas is satisfying, but somehow the real work of art seems to be this new person who created it. The real masterpiece being this person who died on August 17, 2009 and was reborn through his art. | The Right Hand of TherapyI am Cindy’s right hand. Together we learned how to color, how to draw, and eventually how to write. We wrote papers and reports through college and applied to graduate school. Now as an occupational therapist, I am Cindy’s instrument of change as we work with stroke patients in Cleveland, Ohio. We encourage, we console, we comfort, we motivate, and even now, as an experienced clinician, we are surprised to realize how much we learn with each patient that we work with. Throughout our schooling, we always felt that there was so much more knowledge to be gained from a course, a journal article, or a textbook. In fact, we were driven to squeeze every drop of knowledge out of these empirical resources as we could, and we suffered all the cramps and callouses from taking notes to prove it. While we were focused so intently on the clinical outcomes of our patients, we didn’t realize that we were learning from each patient’s experiences along the way. Each patient we worked with would inevitability pave a new course for how we approached treatment with the next patient. So when we saw Bill Forester’s name on our caseload, we did not expect that his treatment would reveal anything new to us. From reviewing his chart and looking at his brain scan, which showed a massive left hemisphere hemorrhagic stroke, we formed general expectations for his plan of care. Left hemisphere stroke likely results in difficulty with language in addition to right-sided paresis and dis-coordination; we already had general interventions and goals in mind that we could start with. When we met Bill, he walked into the clinic with confidence and a half smirk on his face (since his stroke affected his smile and the very sensation of a smile). Our first mission was to get a feel for the patient. He appeared bright eyed and motivated for what was to become an excellent recovery. I could sense Cindy’s thoughts as she observed that he was walking well but that he kept his right arm behind him, as if unaware of where he had parked it. Cindy had me reach out to him, and we took his right hand in ours and began to assess how the stroke had affected him. He had severely impaired proprioception and poor motor skills. He was unable to lift his arm or reach for and grasp an object with his right hand. So we had to demonstrate and show him, our hands on his, how to reintegrate this part of his body back into himself. Though he was not able to speak, it was easy to tell that Bill had an indefatigable personality and strong sense of humor. So that’s where we started. We learned about what Bill had done before his stroke, and set small but achievable goals that would guide us through various interventions. Cindy and I would make Bill walk with us to the coffee stand where the barista, Tim, would give him a cup so that he could pump the aromatic Arabica from the thermos at the self serve station. Tim quickly learned that we expected Bill not only to “order up” his own coffee using his reforming communication skills, but that he had to use his right hand to fill his cup full of that deliciously fragrant coffee. There were blunders of speech and many spills requiring many napkins. Lines sometimes formed behind us and people had to wait. Both Bill and Cindy were determined though, and this never bothered them. They would joke about the mishaps and resolved to do better the next day. Cindy had me always at the ready; available to hold hot “cups of joe” while spills were sopped up, and to prevent Bill from using his left (more functional) hand for the task. Our job was clear; we encouraged Bill through each failed attempt, applauded the successes and supported him when his disconnection between mind and body seemed too much to overcome. Over time and with practice, Bill got better at this seemingly simple task. The coffee from that stand always seemed to taste the best knowing the work that had gone into getting it. As he progressed through therapy, he challenged us to give him more difficult tasks and home practice to improve the strength and coordination with his right hand.
“OK,” I could sense Cindy thinking, “if this guy wants to get more involved, let’s get him more involved.” So I helped Cindy make some calls and we signed Bill up for a 5k community run. We would run it with Bill, and we would be by his side to help him along the way, if he needed it. We could tell that he was hesitant, so we remained steadfast and encouraging. Sometimes we pushed him; sometimes we were the hand on his shoulder steadying him. We reassured Bill that even though his legs felt weak that they would get him through the run, and he would be stronger for it. When the day came, we were there by Bill’s side, but he was the one who took each step that got him to the finish line. And when we crossed that line together, we shared that moment of accomplishment as a team and as friends. I don’t think that Cindy was surprised that Bill completed the run. She might have been surprised however in his interest to train for a marathon at the end of the year because of this first race. He took all of the tasks that we handed him and ran with them. He was challenging us to find new and creative ways to help him reestablish those connections that the stroke had diminished.
“Well, he did so well with that one, let’s keep pushing him,” I sensed Cindy’s mind work. We made a few more calls and arranged for Bill to throw out the opening pitch in a local baseball game. Everyone was supportive once they heard what Bill had been through so it was not a difficult task to arrange. Again, we could sense the reluctance from Bill. It’s funny how much you can communicate with someone even when they can’t speak very well. So we began to practice. It was slow and clumsy work at first. We took his right hand in ours and we helped him relearn how to hold the baseball. There were so many frustrations. His hand resisted but his spirit was tireless. We tried to match his gregarious personality and constant striving to be able to do more with novel strategies that required him to find original solutions to each problem he encountered. We got him used to the weight and texture of the ball and we guided him through the motions over and over again. We started to see Bill improve. We were able to back off to where we guided him from his shoulder, and then we were only there for occasional balance checks. When the day came, Cindy and I supported Bill from the sideline. Again, Bill would have to take this last step on his own. Bill seemed surprised that he was able to make the throw correctly. We thought it was inevitable. In his case at least, hard work had paid off.
Bill was a unique patient who challenged us to deliver dynamic rehabilitative interventions beyond what we had read about in our textbooks. We helped him nurture the critical connection between his mind and body that his stroke had interrupted. In doing so, we formed a strong bond of our own between patient and therapist. He opened our eyes to the challenges that stroke survivors experience at home and during each step of the long recovery process. We saw him struggle with his inability to return to the work that had meant so much to him before the stroke and we were with him as he re-evaluated his next steps in life. We guided him as he confronted his inabilities following the stroke and supported him as he found the capacity to create and live as an artist and a painter. Anyone that meets Bill will recognize his kind spirit and affable determination. Most likely they will marvel at his enthusiasm for life and his perseverance in all tasks great or small. Cindy and I, for our part, will carry the lessons that we learned from Bill to all of our future patients. The most important lesson perhaps, that we allow ourselves to be open to learn with and from our patients as we take their hands in ours and guide them back to themselves. |
 |  |









{kind=link}
About the Artist

Ted Meyer is a nationally recognized artist, curator and patient advocate who helps patients, students and medical professionals see the positive in the worst life can offer. Ted’s 18-year project “Scarred for Life: Mono-prints of Human Scars” chronicles the trauma and courage of people who have lived through accidents and health crises. Ted’s paintings have been shown around the world, from Europe, to Asia, and throughout the United States. With subject matter ranging from introspective, to down-right humorous, his narrative always looks at human interactions.
Ted has been featured on NPR and in the New York Times, Washington Post, Chicago Tribune, and USA Today. His work has been displayed internationally in museums, hospitals, and galleries. As the former Artist in Residence at UCLA Geffen School of Medicine, Ted curated exhibitions of artwork by patients whose subject matter coincides with medical school curriculum. Ted has curated shows by artists challenged by MS, cancer, germ phobias, back pain, and other diseases. In addition, he is a Visiting Scholar at the National Museum of Health and Medicine, and was recently invited to take part in the Aspen Seminars at the Aspen Institute.
The Ted Meyer Story

People often ask me: “How did you land up being the Artist in Residence at a medical school?” Is it really so unbelievable that the guy who wrote and illustrated a children’s book about cats titled “The Butt Hello” could have anything to add to a discussion at a big deal medical school?
When I look at all the different aspects of my life, the outcome seems quite logical. Multiple stays in the hospital, the lady with the art cart, drawing in my hospital bed, the ease I feel in a hospital, all were a part of a clear path. I see these pieces as a path, directing me from the disappointment my parents felt when I announced I wanted to be an artist, to serving as artist in residence at UCLA’s Geffen School of Medicine for the past 5 years, and now onto USC Keck School of Medicine to develop a larger program starting in the fall of 2016.
I was born with Gaucher Disease, a rare genetic illness. I lived through multiple childhood hospital stays and spent years painting pain, loneliness, and fatigue. I got really good at it. Pain as a subject suited me. I might not have sold a lot of my contorted skeletons, or angry figure paintings. But, I got good press. My paintings were getting shown. I showed work from coast to coast. Gaucher had provided me a never-ending source of artistic motivation.
Other than my failing health, everything was going well. That is, until stupid western medicine butted in with a treatment that offered to end my pains and extend my life expectancy to that of a “normal” person. In a single biotech miracle, some faceless pharma company stripped me of my artistic direction. Life-saving drugs left me doing paintings that were no longer about suffering or angst, but love and happiness. It was enough to drive a healthy guy into depression.

I spent a year or two in artistic purgatory with no real vision. Until one night, at an art gallery, I met a lovely wheel chair user. She was sporting a long scar on her back that she showed off proudly in a backless dress. Her name was Joy and she was a joy; a real human homonym. We discussed art and our changing life situations. How at that point we were moving in seemingly different directions. I was getting more active, and she, less mobile. The interesting thing was that she was actually expanding her life. She was cast on a TV show and started working with a dance company to add rolling to their vocabulary of standard dance moves. She told me that although I was now healthy, I should still be doing work about health and mobility because it was all still part of me.
I mulled that over for a bit, and because she was really beautiful, I thought she might be right. I called her that night and asked if I could make a contact print of her scar as a way to tell her story. So I showed up at her house a few hours later with ink, roller and paper and made the first print in my Scarred for Life series. A long blue imprint that clearly showed incision, stitching and the unnatural bend in Joy’s back where it had been broken.
At the first opportunity I showed Joy’s scar along with those of two other people. The reaction was unexpected. Gallery goers, normally more interested in cheese squares and wine, lined up to discuss the print as well as tell me of their scars. I heard stories of accidents, operations and violence. People unbuttoned shirts and pulled down pants, they practically undressed in the gallery while giving me details of their strength and survival, all the while pointing to their scars. It was like nothing I had experienced. I came to realize that there was a BIG need for scar victims, even those considered done with their recovery, to tell their stories to complete their healing. They needed recognition of their struggles, and of survival.
For the next 12 years I collected scars, and I collected stories, and made prints. I heard tales of operations and recovery, of organs removed and replaced, arms and legs lost to nature and autos. During that time I learned that the people who landed up in my studio were not defined by their traumas or missing body parts, they were instead an amalgam of pre- and post- scar narratives; both aspects linking together over the scar to create a new meaning of the experience and of their lives.
I listened to my scar models’ histories, I heard about their medical care and about doctors who were fantastic with a blade, yet less fantastic with their bedside manner. I thought of my own medical care and the doctor, a wiz at sports medicine and joint replacement, who brought a group of med students into my room to show them “his scars” (a result of a my bi-lateral hip replacement). He was excited to show them how neatly “his scars” had turned out because he did such a skillful job. I know it was just semantics but it was on my new hip, and it was my skin, so I sort of thought of it as my scar, however he clearly took ownership of my body.
With my mixture of personal stories, first-hand accounts, and a love of art, I thought, what can I do with all this to change the doctor/patient discussion? Could I get doctors to see their patients as I did? As people with developing stories accented by treatment or trauma that kept unfolding years after treatment might have finished.
I thought if I could get to the students early, when they were still learning the art of medicine, I might be able to affect a change in how they looked at their patients. I came up with an idea to bring art by patient-artists into the medical school and tie their work to what was being studied that quarter. For example, if the students were looking at the respiratory system I might find an artist with Asthma. An artist who was shot in the brain would cover neurological. Shows on back pain, cancer, migraines, dementia and adult disabilities followed. I’d give them gallery shows and arrange a Q & A with the students and direct the artists to explain how their medical conditions motivated them to make art; how experiencing their particular illness, rather than limiting their lives, actually expanded their artistic horizons.

With a great deal of patience and perseverance I was finally able to get in touch with the Dean of Education at the UCLA Geffen School of Medicine. I told her my idea of a patient-artist gallery as a learning tool for the school and within 20 minutes I had an appointment for the next day to come in and pitch my program.
Five years later, after 19 shows featuring 23 artists and garnering fantastic press, what have I accomplished? As an artist and curator I have given a lot of artists a showplace for work that normally would be hidden. It is generally accepted that art should be about something… until it is. Then people want to see a sunset. Work about cancer, bipolar disorder and electro shock therapy, no matter now beautiful, generally does not get shown in the art world. I’ve created a venue for art with a strong personal medical narrative.
Then there are the medical students. Did I reach my goal of getting them to think differently about their future patients? Yes, I hope so. I hope that the effects of such learning in the short term is of broadening a student’s horizons, to allow them to investigate outside the boundaries of what has been traditionally defined as the world of medicine. The longer term effects are upon the creation of a sensibility that allows for the unknown to exist, for humility to develop towards a patient’s experience.

Dominic Quagliozzi, an artist with Cystic Fibrosis creates artwork about his repeated hospital stays actually using his hospital time to make new work about his ordeal. His work expresses the boring routine of repeated hospitalizations. During his talk you could have heard a pin drop as he explained, and showed in his paintings, what it was like to live life on a waiting list for new lungs. Susan Trackman, an MS patient talked about losing control of life while showing the intricate patterns she makes from all her spent medical vials. “The only control I have over my medical life is what patterns I make with all the junk it generates,” she said.
Art has kept me sane during my life with Gaucher and it has given others insight into what I go through. It has worked for me and I know it works for others. I know that compelling art can teach new doctors a lot about the conditions they will be treating
My long-term goal is to expand my program to other medical schools. There is no reason these shows can’t travel from school to school with matching educational materials.
It is an opportune time to be doing this work, as the field of Health Humanities, Narrative Medicine, and the number of visual and performing arts programs in major medical schools continue to grow. The climate of medical practice and the healthcare system is undergoing a radical change, with major governing bodies like the ACGME and AAMC amongst others charging the field of medical education with the radical proposition of training doctors who are reflective and humanistic as well as technologically savvy.
Scarred for Life Project
For over 18 years Meyer has been creating a graphic yet beautiful depiction of people’s suddenly altered bodies and the resulting scars in an ever-enlarging collection of artworks entitled, “Scarred for Life.” “Scarred for Life” continues to grow and now consists of almost 100 artistically enhanced monoprints taken directly from the scarred skin of his subjects. Each image – accompanied by a photographic portrait taken by Ted and a written story by his subject – tells a unique and intriguing story of medical crisis, resilience and healing.
The project’s title embodies a duality of ideas that are explored in depth: first, that medically related scars or physical disfigurements often have a profound lifelong impact on a patient’s self-identity, and secondly, that those scars have the potential to serve as powerful symbols of regeneration and life, and learning tools as well. Exploring facets of self-adornment, contemporary trends in body modification and the ways in which art has been used to redefine aesthetic norms, Scarred for Life presents ways in which medical patients can grow to view their scars as beautiful symbols of personal resilience.
Meyer has recently joined up with Dr. Simi Rahman, a pediatric hospitalist and educator at the Keck School of Medicine at USC in Los Angeles to expand the scope of the work and to add educational and professional rigor to it. We have started www.artandmed.com with a full list of talks and workshops and interviews with artists-patients being added all the time.

This work is licensed under a Creative Commons Attribution 4.0 International License.