The Intersection of Science, Medicine, and Art
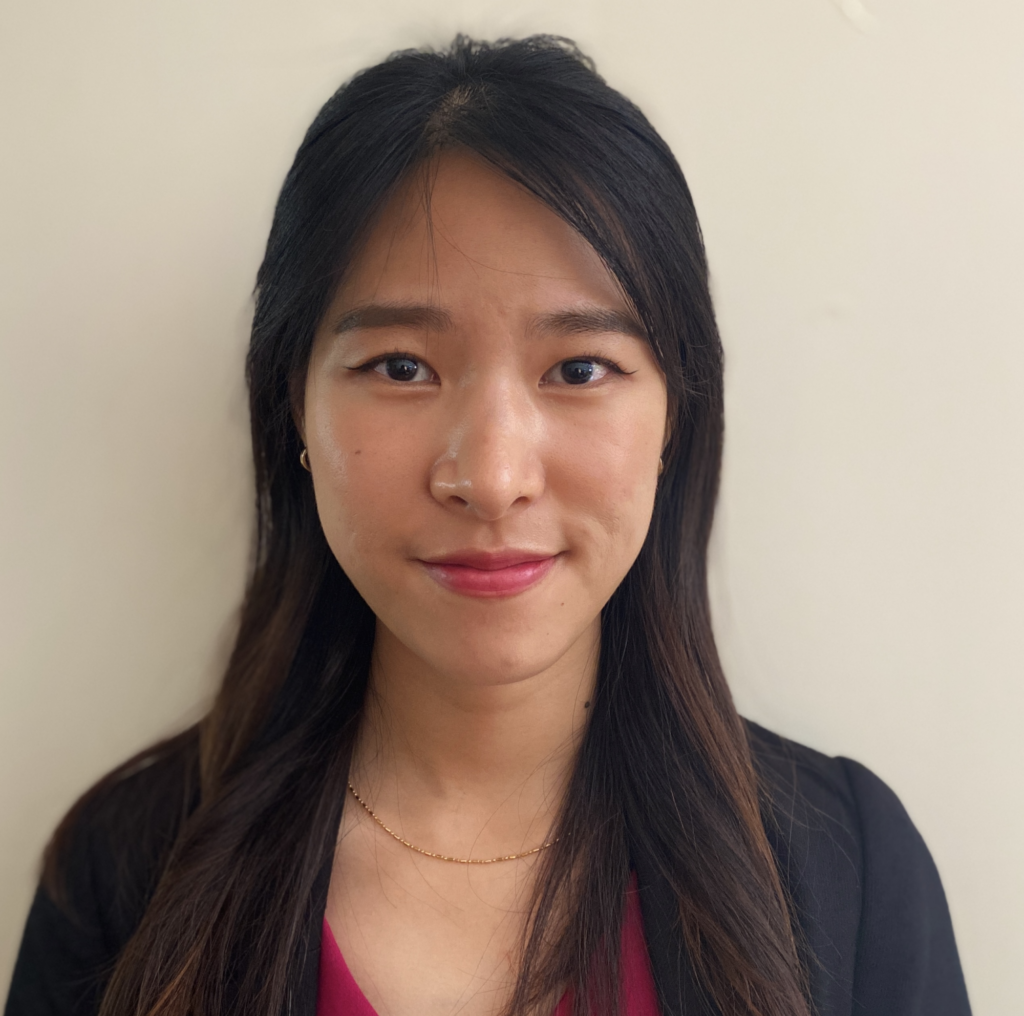
On a recent Wednesday afternoon, a pair of first-year students from the Philadelphia College of Osteopathic Medicine stood in front of one of Henri Rousseau’s dreamlike, allegorical portrait paintings in gallery 19 at the Barnes Foundation. Provided with a detailed exercise sheet, and working independently, they had been instructed to take 10 minutes to consider: “Who are these people? What are they doing? What is their relationship to each other?” They were also asked to be aware of: “What aspects of the picture led you to draw your conclusions? What in the painting supported those conclusions? And with what level of confidence?” Finally, they were asked to consider: “To what degree are your conclusions influenced by inferences or interpretations that went beyond what you could concretely verify in the painting itself?”

The students were then asked to take another 10 minutes to consider the image from an alternative point of view: “What other conclusions might be drawn from the same image? What else might be happening? How else might you explain what you see?” and “What would you say?” Partners then discussed their interpretations with each other, taking note where their conclusions were similar and where they differed.
Elsewhere in the collection their fellow classmates were considering the same questions with other pictures. Finally, the full group of 20 students gathered in a classroom where pairs reported on their experience, explaining to their classmates what they thought and why. After an animated conversation, the session concluded with each participant writing about their experience in a journal, reflecting on the exercise and the conversation that followed.
Why were medical students spending two hours in the middle of the school week looking and discussing works of art? They were participating in the Barnes Foundation’s Art, Well-Being and Medicine program, which uses the collection to explore topics and concepts relevant to medical education, clinical practice, and overall well-being. For instance, how might close looking at a painting help hone diagnostic skills? Or can discussing a work of art with a partner as well as a larger group enhance effective communication?
The fact that this program was taking place at the Barnes Foundation was no mere coincidence; the intersection of science, medicine and art is central to our institutional history. Following is a brief account of our founder’s path to the creation of the Barnes Method of art interpretation.
Albert C. Barnes: Education as a Path From Poverty
Albert Combs Barnes was born in 1872 to a family of modest means in the highly-industrialized Kensington section of Philadelphia. His father, John Barnes, had sustained a debilitating injury fighting in the Civil War. Early in Albert’s childhood, his father’s inability to hold steady employment forced the family to move from Kensington to a particularly rough section of South Philadelphia known as “The Neck.” Despite these trying circumstances, young Barnes excelled at school and was accepted to Central High School, which had a national reputation and was empowered to give advanced degrees. Having earned a Bachelor of Arts degree, Barnes matriculated to the University of Pennsylvania, where he graduated with a medical degree in 1892 at the age of 20. Education provided a pathway for young Barnes to move from poverty into the medical profession.
Rather than practice medicine, Barnes worked as an advertising and sales manager for the pharmaceutical firm H.K. Mulford and Company, spending extended time in Europe. While there, Barnes and his business partner Herman Hille developed a silver-based antiseptic compound designed to treat eye inflammation, especially in infants, which they named Argyrol. Barnes and Hille formed a partnership for the manufacturing of Argyrol and soon moved production to Philadelphia. They dissolved their partnership in 1908, and Barnes established the A. C. Barnes Company, taking over sole production of the product. Under his guidance, Argyrol became widely administered—making Barnes a wealthy man.
With this wealth, Barnes began collecting art. In 1912, he convinced his friend and fellow Central High classmate William Glackens—by then one of America’s most respected avant-garde painters—to go to Europe with a line of credit. The mandate was to purchase the best examples of modern paintings he could acquire. Glackens returned with more than 30 works of art, including paintings by Pierre-August Renoir, Paul Cezanne, Camille Pissarro, Vincent van Gogh, and Pablo Picasso.1 Many works from the Glackens acquisition remain in the Barnes today, forming the foundation of one of the country’s most important collections of early modern art.


A Commitment to Education
For a male, white, upper-middle-class business owner at the turn of the 20th Century, Barnes was both socially progressive and steadfastly committed to the personal and professional power of education. In his West Philadelphia Argyrol laboratory, he hired African American men to work the laboratory floor and white women as office administrators. Barnes organized the business as a cooperative, encouraging personal growth and a spirit of mutual respect among his employees. Recognizing that the amount of product needed to satisfy sales could be produced in less than eight hours, he began to set two hours of the paid workday aside for his staff to meet as a group. They read and discussed works of literature, history, and philosophy—and looked at and discussed the modern art he was collecting and hanging in the Argyrol laboratory.
One of the texts discussed in these laboratory seminars was John Dewey’s How We Think published in 1910. Impressed by Dewey’s philosophy of pragmatism and deep commitment to democratic means, in Fall 1917, Barnes enrolled in a post-graduate philosophy seminar taught by Dewey at Columbia University. Despite their dramatically-different personalities, Barnes and Dewey became close friends and confidants, remaining so for more than three decades.2
Inspired by Dewey’s philosophy of experiential education, Barnes resolved to formalize the educational experiment begun in the Argyrol laboratory. In 1922, Barnes chartered the Barnes Foundation with the Commonwealth of Pennsylvania as an educational institution dedicated to promoting the appreciation of fine art and arboriculture. (Barnes’ wife Laura was an enthusiastic horticulturalist.)
From Idea to Reality
That same year, Barnes purchased a 12-acre parcel of land in Merion Station, Pennsylvania from Captain Joseph Lapsley Wilson. For more than 50 years, Wilson had collected and cultivated over 200 specimens of trees—establishing one of the country’s first arboretums. Barnes hired the French American architect Paul Philip Cret to design a gallery building and attached residency, to be built within the arboretum. In 1940, Laura Barnes and botanist John Milton Fogg Jr. of the University of Pennsylvania began the Arboretum School of the Barnes Foundation.
With John Dewey as the honorary director of education, Barnes welcomed the first class of students to the Foundation in 1925. The collection by then also included one of the largest personal collections of art from African cultures in the United States displayed alongside works of American and European modernism. The opening of the Foundation was the realization of an educational trajectory that had lifted Barnes out of poverty in Philadelphia’s neighborhood “The Neck” through Central High School and the University of Pennsylvania to opening educational opportunities for anyone with a genuine interest in learning about art and its connection to lived experience.
The Barnes Method: Scientific Methods + Art Analysis
Exploring the relationship between art and the everyday is central to another project that Barnes pursued as his collection grew. Dissatisfied with contemporary methods of art history and analysis, Barnes found it necessary to develop an analytical framework for his own understanding and evaluation of art. Adapting aspects of formalism promoted by Roger Fry and Clive Bell, informed by the pragmatic philosophy of John Dewey and William James, and structured on the scientific methodology of his own medical education, Barnes developed what he called an objective method for art analysis: what we today call the Barnes Method.3
Strongly object-centered, the Barnes Method relies on close looking and critical thinking focused on the art object itself. Observation and analysis concentrate on a work of art’s visual qualities, such as the artist’s use of color, line, light, and space. Observations are made and suppositions proposed. These are measured back against the art object and refined, revised, or rejected. The combined effect of confirmed observations helps inform a culminating conclusion as to the work’s expressive effect. Conclusions are grounded in concrete experiential qualities. For example, a painted area may convey a sense of solidity, three-dimensionality, weightiness, set-ness, and containment. A still life by Cezanne, for instance, may express qualities of precariousness or instability, as objects with the above qualities are set on the inclined plane of a tabletop.

Drawing expressive conclusions rooted in concrete, objective, experientially-based observations is a distinguishing characteristic of the Barnes Method. This clearly separates it from, say, Roger Fry’s formalism, which focuses exclusively on an analysis of a work of art’s form. In addition, the Barnes Method encourages objectivity, not allowing personal subjective preferences to influence critical judgement. Instead, the Method asks viewers to put aside individual likes and dislikes, and, to the degree possible, evaluate an object with clear unbiased reasoning.
Pursuit of objective analysis is one important way that the Barnes Method supports the relationship between art and medicine. For instance, how can analyzing a work of art, learning to see beyond an initial response to its subject, focusing instead on aspects that are concrete and verifiable, then finding language to describe our perceptions to others, relate to and perhaps improve diagnostic and communication skills in medical students and clinicians?
The Barnes Method in Medical Education
It was against this historical background that in 2018 work began on developing a program that would use the collection and methodology to explore issues and topics relevant to medical education, clinical practice, and overall well-being. The Barnes, with its collection of paintings, sculptures, furniture, wrought iron, textiles, ceramics, and other objects arranged in unique juxtapositions called ensembles, creates an unexpected environment for learners.
The varied size of gallery spaces and the range of objects drawn from global traditions, including a diverse collection of decorative arts, provide a rich and complex source of visual experiences. The collection functions like a laboratory ideal for exploring the interrelationship between aesthetic experiences with works of art and the lived experiences that fill our everyday lives. With their multivalent interpretations, the ensembles continue to challenge expectations and frustrate simple explanations. Learning within this space offers unique opportunities to cultivate critical thinking skills and gain valuable insights into patients with complex diagnoses and recovery journeys.

Some may argue that medicine and art are antithetical—that medicine deals with science and facts and art deals with feelings and emotions. However, there is a large and growing body of research that shows multiple benefits of integrating the humanities into medical care and education.4 The gallery space can be a neutral environment for considering issues related to medical education and overall well-being while developing transferable skills for clinical practice.
Guided Experiences for Practitioners – and Patients
Guided experiences with works of art can provide medical students and early-career clinicians the means to confront challenging topics and improve interpersonal skills.5 As a medical professional progresses in their career, the benefits of spending time in art galleries can evolve to become a means of self-care helping to combat burn-out.6 Professions with high levels of stress, such as medical ones, experience increased rates of burn-out—a trend that dramatically increased during and in the wake of the COVID-19 pandemic. Research published in 2022 in the journal Mayo Clinic Proceedings, showed that 63% of physicians surveyed reported at least one symptom of burnout at the beginning of 2022—an increase from 38% two years earlier at the beginning of the pandemic, and compared to 44% in 2017 and 46% in 2011.7
Time spent in gallery spaces like the Barnes can have physical benefits for all—and patients in particular. Research8 has found that museums create value by catalyzing feelings of wonder, interest, curiosity, enhanced understanding, a greater sense of belonging, and perceptions of physical safety and serenity. Value is rooted in the ability of museums to use their collections in ways that make accessible to a broader public vast and diverse knowledge about the past, insights into present-day cultural identities, and opportunities for the creation of future creative expression—all of which are made manifest through the varied experiences that art collections support.
Research has shown universal well-being-related value across five dimensions (personal, intellectual, social, emotional, and physical) that are strongly correlated with perceptions of a satisfying and successful life.9 A vast majority of the public perceives that they derive universal benefits following a museum visit, indicating that these museum experiences have societal value of a duration of several days or longer.10
Art as Prescribed Treatment
After visiting art collections like the Barnes, a large majority of the public experience personal, intellectual, social, emotional, and physical well-being. And these universal benefits are strongly correlated with perceptions of a satisfying and a successful life. In the United Kingdom, doctors experimented with prescribing “therapeutic art or hobby-based treatments for ailments ranging from dementia to psychosis, lung conditions and mental health issues.”11 Doctors in Brussels prescribed museum visits to their patients who were struggling with stress due to the COVID-19 pandemic, with the hope of “alleviating symptoms of burnout and other forms of psychiatric distress.”12
Research conducted by colleagues at the University of Pennsylvania’s Positive Psychology Center suggests that “art museum visitation is associated with reductions in ill-being outcomes and increases in well-being outcomes.”13 It was in this environment of growing interest in connecting medical students, professions, and the broader public to the humanities that the Barnes began developing the Art, Well-Being and Medicine program.
The Art, Well-Being and Medicine Program at the Barnes Foundation
The Barnes Foundation was approached in 2017 by Dr. Sheldon Weintraub and his wife Margie who were interested in creating a legacy gift in Sheldon’s name. Sheldon, a retired physician who had trained as a Barnes docent, was in the last stages of terminal cancer. As a docent, Sheldon would occasionally welcome fellow physicians to the Barnes; together they would discuss the relationship between experiences they had with works of art and the practice of medicine. Building on these experiences, Sheldon and Margie created the Dr. Sheldon Weintraub Fund, which provided funding to support the development of the Art, Well-Being and Medicine program.
Simultaneously, Adrian Banning, an instructor in Drexel University’s physician assistant (PA) program, reached out with an interest in bringing first-year students to the Barnes for an art and medicine experience. Working with Banning and colleagues at Drexel, the Barnes program designed a series of gallery exercises around key concepts. Topics were chosen and researched, materials were workshopped to determine appropriate language and gallery experiences, curricular relevancy was determined, and related supporting materials were identified.
Six gallery-centered exercises were initially designed, with one added a year later. They are:
- Close looking. Exploring how spending time looking carefully at a painting might relate to clinical diagnostic skills.
- Critical thinking. Moving beyond set assumptions to deliberately and methodically explore problems or situations.
- Clear communication. Promoting a skill important between physician, patient, and family but also across the medical field and beyond.
- Collaborative problem solving. Emphasizing medicine as a team effort; valuing all voices and perspectives for a team to function effectively.
- Building empathy. Being open to truly hear and respond to others, or as Rita Charon, MD, PhD, and developer of narrative medicine writes, “the ability to acknowledge, absorb, interpret, and act on the stories and plights of others.”14
- Developing self-awareness. Recognizing both one’s personal skills and strengths as well as limits and biases in order to minimize the over-influence of either.
- Navigating ambiguity and addressing uncertainty. Focusing on building personal decision-making strategies in the face of potentially competing or conflicting outcomes. This exercise was added a year after the program began, on the suggestion of a returning third-year Drexel PA student.
Importantly, each exercise is accompanied by literature drawn from respected medical journals that supports and validates the exercise topic. In addition, colleagues at Drexel’s PA program contributed concrete examples of clinical relevancy outlined on each exercise document. It was essential that the experiences be enjoyable but also meaningful. Exercises were also intentionally designed to provide returning participants a variety of experiences.
Participants may work as a large group, but also in small groups, pairs, and individually. Among the program’s requirements:
- Participants are required by the exercises to engage in dialogue with their colleagues—sharing experiences and perceptions.
- Participants are also asked to make presentations to their colleagues, requiring their thoughts and ideas to be organized and clearly articulated.
- Groups participating in multiple visits are asked to engage in written reflection through journaling at the conclusion of each session. Between sessions, these participants are prompted to read their previous entries, reflect on them and the time between, and write more. Journaling allows participants to translate vague impressions into concrete ideas; their journal becomes a record of their evolving experience.
Example: The Rousseau Painting and Addressing Uncertainty
One topic that surfaces in nearly every Barnes program session is navigating ambiguous or uncertain situations. How are conclusions reached when more than one outcome appears equally valid? How are decisions made in the absence of all desired information?
…Which brings us back to our pair of PCOM medical students in gallery 19 and questions regarding the Rousseau painting (Fig. 1)—such as, “Who are these people? What is their relationship to each other? What is going on?” Paintings are ideal for addressing issues like this because they are very often themselves ambiguous. They present some information very clearly, but what that information adds up to is often unclear.
In the painting in question, a man and woman dressed in formal black clothes stand next to one another, exchanging a bouquet of flowers. They are in a wooded landscape behind a small flowering shrub and sinuous vine. This seems fairly straightforward. Yet, in the sky above, floating among the clouds, are the disembodied heads of a man and woman. Who are they? What relationship do they have with the standing pair? What is going on? And what is the relationship between the two standing figures? Are they brother and sister, wife and husband, or something else? Here the painting is opaque. Answers to these questions are not clear. We are left to decipher it as best we can.
Addendum. Rousseau painted this picture in 1899, the year after he married his second wife Josephine Noury. Both had been widowed; the heads in the clouds represent their former spouses, who Rousseau shows blessing the new union. However, this meaning is not clear from the painting itself. Rousseau’s inventive composition is open to various interpretations, making it ideal for this exercise. Rousseau was a self-taught artist.
Conclusion
Building a Repertoire of Tactics
Confronting challenging topics in a neutral space like an art gallery, where no real-world consequences exist, allows participants to focus on the process they undergo without concern for potential outcomes. They are free to test approaches and cultivate personal strategies, building a repertoire of tactics that they may draw on when needed in real-world situations. Programs like the Barnes’s Art, Well-Being and Medicine provide space and guidance to help participants develop important personal and professional skills.
Strengthening Well-Being
In addition, spending time in collections like the Barnes can build a greater level of comfort in this and similar spaces, particularly for those unfamiliar or naturally unsure in art collections. Upon concluding their participation in the Barnes’s Art, Well-Being and Medicine program, we hope participants will want to return to spaces like these for their own well-being.

![]()
This work is licensed under a Creative Commons Attribution 4.0 International License.
Medical school can install students in locales both familiar and unfamiliar: the darkened hush of a lecture hall, the sheeted tables of an anatomy lab, the beeping monitors crowding an ICU. But students may now also find themselves before a Pollock or a Kahlo, contemplating art in the vaulted halls of a museum exhibit. Medical schools are increasingly partnering with museums to formally integrate the arts and humanities into their curricula. Recently, I had the opportunity to pilot such a program—a visual arts elective at Emory University, called “Outside the Frame.”
Museum-based education is far from a new phenomenon in undergraduate medical education (UME), but many such programs rely on the sole use of Visual Thinking Strategies (VTS), a facilitated method of guiding students in analyzing an art object. VTS employs three main questions to achieve its aims:
- What is going on in this image?
- What do you see that makes you say that?
- What more can we find?
Through articulating their ideas and grounding them in heuristic evidence, students learn to continually revise their interpretations while building on the viewpoints of others. Ample evidence exists in the literature that VTS in health professions education can effectively enhance observational skill, communication, perspective-taking, critical thinking, and empathy.1,2,3
Context: An Underexplored Area
While true that a minimalist approach to VTS allows educators across institutions to more easily adopt its pedagogy, this strength simultaneously forecasts a key weakness: the tacit assumption that art can be accessed through visual cues alone. VTS can serve as a useful starting point to grease the skids and usher students into a space of inquiry; however, current imaginings of museum curricula in many UME programs abstain from elevating the role of context to explore the pedagogy’s full potential. A proposed fourth question for VTS:
- What contexts may lie beyond what we see?
Although a context-free standard may nurture an appreciation for multiple perspectives and avoid premature closure, it also arrives at this point by intentionally disaggregating from any historical, social, political, or ethnographic background that could potentially imperil an “open” reading of the work. In so doing, it not only deprives itself of the opportunity to interact with the diverse disciplines intersecting in the museum space that can advise on such topics, but also denies students the ability to productively engage with context.
Triangulating Perspectives
Far from just a geographic or physical setting, context refers to the varying conditions and ideologies under which our institutions function, from hospital funding to heteronormativity. As the COVID-19 pandemic has sufficiently foregrounded, the increasing complexity of healthcare challenges us to honor these contexts by adapting a curriculum from an objective, metrics-based approach to a more “systems”-based one that can triangulate data and perspectives from multiple sources.
Beyond cultivating students’ diagnostic skills and building outsized reliance on individual powers of observation, modern medical training needs to encourage students to engage with unfamiliar contexts outside the boundaries of personal experience. By considering the specific academic codes, debates, and practical frameworks of art history and other social sciences disciplines, students could venture more confidently beyond the primacy of their medical training and integrate knowledge from a broader disciplinary toolkit. Such an approach would allow learners to re-envision uncertainty as not merely something to be ‘tolerated’ but actively explored as an essential source of intellectual curiosity—something of which medical trainees have no shortage.
Our Multidisciplinary Approach
Our curriculum, therefore, actively sought out and queried outside expertise from faculty broadly ranging across multiple departments, such as art history, classics, psychology, and history. In our final session, we gathered in the conference hall at the Carlos Museum, where art history professor and curator Dr. Rebecca Stone gave a lecture on shamanism in ancient indigenous art and its role in healing, titled: Plant Teachers, Shamanic Visions, and Death.
I sensed some apprehension in the room as the lecture proceeded, and couldn’t help but feel it myself, having just emerged from a lecture on soft-tissue infections and broad-spectrum antibiotics.

Cast against the absolutizing categories of side effects and dosage requirements, the topic of shamanism seemed impossibly distant and nebulously vague. Gradually, however, I observed students’ reactions to the content transform from guarded bemusement to wonder—as what initially appeared to be an extended non-sequitur began to draw fascinating parallels to relevant clinical material.
The lecture touched on various pieces in the Carlos collection relevant to shamanism, such as the Deer-Human effigy in Figure 1. Hailing from modern-day Costa Rica and Nicaragua, this work depicts a woman in a typical shamanic trance pose, seated with crossed legs and her hands resting on her thighs. On closer inspection, however, conspicuously non-human features emerge: her “hands” have coalesced into dark hooves, and knobby protrusions bud from either side of her head like antler stumps. These features contradict her still-human feet, which are painted directly onto her thighs rather than carved like the hooves, as if her anthropocene characteristics are literally receding into the background in light of her transformation. She reflects an important visual theme common to many ancient American art styles—that of shifting form, usually into animals that signify inhuman physical prowess, like heightened senses, strength, and speed. These qualities codify a larger spiritual shift, considered important especially for shamans as they leave the boundaries of their physical form to navigate the spiritual world.
As Dr. Stone explained to us, shamans are healers who have been ascribed with such powers because they survived, and thus emerged “victorious” from, physical challenges. Having transcended the limitations of the terrestrial, these figures now tread the demarcations separating life from death, male from female, human from animal.4
Another effigy we discussed adopts a similarly-meditative hands-on-knees pose, but with several marked differences: the eyes are slit in a faraway “trance” state, and the head strangely ends in a cap-like top (Fig. 2). Moreover, whereas the former figure had unmistakably female characteristics, this one is more ambiguous, with features suggestive of both male and female gender. Students were then treated to several relevant informational tidbits: 1) that the cap-like head alluded to the characteristic tops of psilocybin mushrooms (Fig. 3) ritually used by shamans for their psychedelic effects; 2) the figure was thought to depict an individual with Klinefelter syndrome, a condition in those male-born with an extra X chromosome.



Noises of excited recognition rose from the group. The brief, bulleted takeaways on Klinefelter’s we had been exposed to thus far had largely been lensed through a Western science perspective, which portrays the condition as a pathology terminating in several unfortunate outcomes: lower IQ, infertility, erectile dysfunction, hunchback, a higher mortality rate. These symptoms, easily summarized by the unsuspecting learner as ‘disfigurements,’ cast a similarly negative pallor on some of its other hallmarks: wide hips, a taller stature, gynecomastia (male breasts), and small testes (Fig. 4).
And yet, to shamanic culture, these were not so much disfigurements as sublime signs of an expanded, transcendent existence—someone who could navigate between the binary constructions of sex. These new factoids not only painted the disease in a new light, but also built on the previously-given information that ingestion of mushrooms was associated with enhanced visionary powers. Importantly, the figure (Fig. 2) was portrayed as not just taking mushrooms, but as being in the process of transforming into one. In so doing, it depicts the shaman as not merely passively submitting to the drug’s influence, but also as metaphorically embodying the drug’s very power and potential.
Context Exposing Prejudice
Learning the context underlying these effigies exposed our occupational prejudices in more ways than one: we were forced to revise our thinking about not only Klinefelter’s as a disease, but also on what such a ‘diseased’ state even implies in our medical culture. A tendency toward classification and closure permits physicians to see patients as a means to an end—to encounter someone as a composite of informational soundbites that must satisfy, and ultimately reproduce, a familiar illness script, narrative, or pattern. The ‘ill’ person thus becomes subjected to the superior ordinance of disease, which decrees a predetermined, biologically-fated outcome that implicitly denies patients their individual agency. But for shamans, disease is not a terminal end-point at which all possibility converges to a halt, but rather a beginning: an aperture through which one transforms, grows fluid, gains new insight and transcends boundaries. What is at stake is not a narrowing down of possibilities, but their broadening—to see further, feel deeper, and journey into new realms.
Reconsidering Ethics of Care
More often than not, modern medicine endeavors to narrow the realm of possibilities. Medicine is a system of categories; when we diagnose a patient, we tend to apprehend them not in their individuality but in their generality, the degree to which their physical description complies with a set of preconceived assumptions and rules. This can be a good thing; certainly, consistency breeds reliability, which is what we want when diagnosing illness, prescribing treatments, or making recommendations. However, this attraction to sameness, to what confirms our bank of pre-existing knowledge, can dangerously skew our ethics of care.
An aversion to the foreign is a part of medical culture. Throughout our training, students are taught to rank the usefulness of their scientific endeavors through the quality of evidence produced. Otherwise known as “evidence-based medicine,” this dogma twins that of VTS in that it largely accounts for detectable presences—of visible signs, symptoms, and outcomes. However, the true reality is that at every stage between observation and interpretation, a scrim of ideologies and values filter through certain features without manifesting the absences—the omitted narratives, the alternative worldviews. A privileging of only that which can be personally seen, inferenced, and proven can lead to a hierarchized view of knowledge production, creating an epistemic gap that siloes and isolates trainees from the fundamentally nuanced and human nature of the work we do.
By exposing students to these unfamiliar cultural contexts, we did not necessarily intend to encourage belief in shamanism, or the valuing of disease as ‘good’ and empowering. Rather, we were trying to show them that the layering of context can expand, rather than restrict, one’s horizons and capacity for interpretation. To understand that other cultures may elevate those we deem ‘unfortunate’ or anomalous can challenge us to suspend our own frames of reference while validating the patient as someone who is also continually deriving meaning from their embodied condition.
As future physicians, trainees must understand that the ‘hidden curriculum’ of medical education lies not in mastering or demonstrating competence in the unfamiliar, but in learning how to invite in, and partner with, this otherness. To take a page out of shamanic culture: the boundaries of self are always only the beginning of the story.
Acknowledgements
The author would like to sincerely thank Dr. Ali Zarrabi and Ms. Elizabeth Hornor for their insight and contributions in coordinating this course.
![]()
This work is licensed under a Creative Commons Attribution 4.0 International License.
Introduction
Horace Pippin began creating art as a hobby in his childhood; this practice later served as an important force in both his physical and mental-health rehabilitation. This article discusses how Pippin’s paintings reflect a range of his experiences and demonstrate the power of art as a form of healing and communication.
Horace Pippin was born in West Chester, Pennsylvania, on February 22, 1888, to Harriet and Horace Johnson Pippin. He was born as a free man 23 years after the official end of slavery. When Pippin was two years old, his family moved to Goshen, New York—but he would return to West Chester in his adult years. He was a descendant of slaves and domestic workers. Pippin began to draw at an early age; however, since his parents were domestic workers, they could not afford basic art supplies. Pippin’s resourcefulness and determination differentiated him from his peers. To find ways around his financial limitations, he participated in several drawing competitions. In 1898, when he was 10, he won a box of crayons in a contest sponsored by an art supplier, which allowed him to continue coloring—an activity he loved.1
Pippin’s artwork, often described as primitive or naïve, became an instrument for the expression of his creative ideas; he said that he was painting what he literally saw inside his head. “The pictures… come to me in my mind,” he said, “and if to me it is a worthwhile picture I paint it… I do over the picture several times in my mind and when I am ready to paint it I have all the details I need.”1 For Pippin, what started as a hobby developed into a tool for personal healing as well as an instrument to speak out against racial inequity.
World War 1: Physical and Emotional Trauma
In June 1917, at almost 30 years of age, Pippin volunteered for the 15th New York National Guard, later renamed the 369th Infantry Regiment and nicknamed the Harlem Hellfighters.2 The Hellfighters eventually became a highly-decorated infantry regiment in World War 1. They were assigned to the 16th division of the French army because many white American soldiers refused to serve with them.3 This was the Jim Crow era, with many state and local laws enforcing segregation; therefore, this response was not unexpected. At this time, US military leadership was predominantly white, and many officers doubted that black people were intelligent or courageous enough to fight. According to the US national archives, it is estimated that of the almost 400,000 African Americans who served in WWI, only about 10 percent fought in battle.2,3 However, Pippin’s regiment did serve on the front lines—with distinction.
The 369th Regiment quickly proved its courage and combat skills. Initially nicknamed the “Black Rattlers” because of the insignia (black rattlesnake) on their uniforms, the French later called them “Men of Bronze” due to their fearlessness during battle.3 It is believed that the nickname “Hellfighters” was given to them by the Germans because of their courage and ferocity. The Harlem Hellfighters spent 191 days in the front-line trenches, spending more time in continuous combat than any other American unit of that size.3
In September 1918, Pippin was shot in the right shoulder by a German sniper. He fell to the ground, bleeding profusely. A French soldier seeking to help was shot dead and fell on top of Pippin, who was unable to remove him. After spending hours in the rain, he was rescued, but he lay on a stretcher overnight, exposed to the elements, before being evacuated to a hospital. The bullet shattered his shoulder; as a result, he spent the rest of his time at war recovering in a French hospital. Pippin was awarded a Purple Heart after his service because of the injuries he sustained in battle. Discharged that year with a steel plate in his shoulder and his right arm virtually paralyzed, Pippin returned to civilian life in West Chester—shattered both physically and psychologically.
Post-War Return to Art: Physical Recovery and an Ongoing Battle
After returning to the United States with a Purple Heart and an Honorable Discharge, Pippin faced yet another battle—that of ongoing racism and segregation. A decorated veteran, he still was only able to get odd jobs. He returned to Goshen with his small pension, no house, no job, and in pain.
However, he found happiness through marriage. He wed Jennie Ora Featherstone Wade, a twice-widowed woman raising her 6-year-old son alone. Jennie’s extended family lived in West Chester, Pennsylvania, so it was an easy decision for the couple to move there to build a life. Although he could not lift his arm above his shoulder and had little strength in his right hand, he helped where he could. Pippin worked at a segregated YMCA, started a Black boy scout troop, and organized an all-Black football team. He enjoyed attending meetings at the American Legion, a non-profit group working with veterans and their families. His love of music led him to create an American Legion drum corps, which he led.
Like many men who fought in the war, Pippin experienced “shell shock,”4 which we now know as Post Traumatic Stress Disorder (PTSD). He was advised to write about his thoughts by other members of the American Legion, but the writing did not calm his mind. He wanted to go back to making art, but he couldn’t hold a pencil in his right hand. One winter as he sat by a cook stove, he picked up a hot poker and outlined a rough image on wood. Through a painstaking and difficult learning process, he devised a method of using his left arm as a support for his right hand clasping a paintbrush. This rough attempt convinced Pippin that he could return to making art.
By 1930, he had begun to teach himself to paint with oils, first on discarded cigar boxes, or by burning images onto wood panels using a hot poker (a technique called pyrography), and then applying oils.
In one of the few autobiographical accounts by a black soldier to come out of World War I, Pippin related his combat experiences in matter-of-fact terms. In books illustrated with pencil and crayon drawings of marching troops, soldiers wearing gas masks, exploding shells, and aerial dogfights, he recorded nightmarish memories of war on the Western Front. Pippin’s compelling World War I notebooks can be viewed online at the Smithsonian Institution’s Archives of American Art.
Art as Therapy
Perhaps unknown to him at the time, Pippin employed occupational (or rehabilitative) therapy practices (treatment of injuries, illness, or disabilities through the therapeutic use of everyday activities) in his quest to restore his war-broken mind and body. Painting, for him, became a means of therapy for his horrendous memories of war, and a way of dealing with his paralyzed extremity. Pippin’s postwar notebooks, letters, and journals, now housed at the Archives of American Art, Smithsonian Institution, explain his experiences after his return home from war, and make clear the importance of art in his life. “When I was a boy I loved to make pictures,” Pippin wrote, but war “brought out all the art in me… I can never forget suffering and I will never forget sunsets. So I came home with all of it in my mind and I paint from it today.”5
Pippin’s Timeless Imagery
Before departing for World War I, the Harlem Hellfighters were refused permission to participate in the farewell parade … known as the Rainbow Division because they were told that black was ‘not a color in the rainbow.’3 Their extraordinary courage in battle earned them fame in Europe and America, with multiple members of the regiment receiving awards from the French and American governments. After they returned home, they were rewarded with a victory parade. New Yorkers of every race showed up in large numbers to celebrate the Harlem Hellfighters as they marched up Fifth Avenue in Manhattan. However, this newfound fame did not last long. The story of the courageous Harlem Hellfighters has largely been erased from the awareness of Americans and the world.3 The story of the Harlem Hellfighters is not widely discussed in contemporary American culture. The works of Horace Pippin celebrate this history and draw national attention to these heroes.
Truth From the Front Lines
Nearly 15 years after he returned home from the war, Pippin created the painting The End of War: Starting Home (1930) (Figure 1). In this painting, Pippin condenses the terrifying episodes of war documented in his journals, showing images of combat fear, battle, and most importantly, the surrender of German troops. He included images of tanks, guns, hand grenades, gas masks, and other tools of war, alluding to the technological advances that made the war more brutal than any before it.6

Perhaps the most important part of this painting for Pippin is his depiction of the African American soldiers. Pippin painted them to almost blend in with the background; perhaps this was his way of depicting how the efforts of African Americans in the war were often overlooked and given little recognition. They fought for a country that didn’t seem to appreciate their efforts even though they had proven themselves as American heroes and worthy soldiers.
A Direct and Powerful Statement
The painting Mr. Prejudice (1943) (Fig. 2), would become what is Horace Pippins’ strongest and loudest statement about racial inequality in the US. Deeply affected by his experiences as a soldier in a segregated troop during World War I, and the poor treatment he and other African American troops received after they returned home, Pippin was moved to make this painting when he noticed that this treatment of African American soldiers persisted into World War II.7

At the top of the painting is a menacing white man with an axe above the “V.” The “V for victory” was a gesture and phrase coined by Winston Churchill during World War II that took root in the US, especially after the bombing of Pearl Harbor. In the African American community, this became a double V, which represented victory in the military conflict abroad as well as the racial conflict at home. The axe held by this menacing white man has created a crack in the V, which divides not just it but the entire painting equally in two. To the left of the painting are African American symbols and to the right, the realities they faced due to racism. To the left of the painting is a black Statue of Liberty, which signifies the freedom and liberty that African Americans have been denied.
At the base of the V is an African American machinist to the left and a white one to his right with their backs turned to each other. In the bottom left, there are four African American men: a doctor, a naval officer, an aviator, and an infantryman (from left to right). To the right of them are three white men who are also involved in the war but are facing the African American men like they need to keep an eye on them. Also seen to the right of the V in this painting is a man in a red shirt holding a noose (a reference to the lynchings faced by Black people during this time) and staring intensely at the Statue of Liberty. Right above him is a person in the signature white robes of the Ku Klux Klan—a group whose numbers increased dramatically in the US after World War II.
This painting shows the dramatic contrast and dangerous circumstances that made up the lives of African Americans during this era.8 Through it, Pippin illustrates what life was like, and the hope of what it could be, calling for liberation and a better existence for African Americans through cooperation between races.
Post-War Return to Art: Scenes of Everyday African American Life
In the nineteenth century, the legal status of African Americans underwent radical changes, they were freed from slavery and began to enjoy some rights as citizens. Despite these changes, many demographic characteristics of African American life were no different from the mid-1800s. At this point, three-quarters of black households in the US lived in rural areas.9 Parents worked on farms with their children, who were very unlikely to attend school. By the late 20th century, African Americans had become less concentrated in the rural south and had better jobs but were still relatively disadvantaged in terms of education, labor-market success, and home ownership. 9 The wealth gap between whites and blacks continued to reflect historical patterns. African Americans struggled to acquire wealth, which made it harder to buy homes, especially due to real estate discrimination. They lived in poor neighborhoods, in houses in terrible condition.9 Horace Pippin’s 20th-century paintings reflected this reality.
Racism’s Effects Brought Home
In 1940, Horace painted Supper Time, an intimate description of everyday African American family life (Fig. 3).

Burnt onto repurposed planks using a hot poker before color was added, this laborious process replicates the hardship depicted in the painting. The image shows a man and a child sitting at a table while a woman seems to be serving them a meal. There is a frying pan sputtering in the background and clothing hanging on a line to dry in the humble home. The house in the painting was made of mismatched planks, depicting the poverty that prevented African Americans from adequately repairing their homes. Pippin brilliantly uses color to guide the eyes of the viewers across the painting. From left to right we see white clothes hanging on a line, a child in white clothes, white cups and plates, and a woman in a white apron and scarf. Pippin also contrasts the pink shirt on the man with the blue dress on the woman. The woman’s dress contains dark shadows in her underarm area, suggesting repetitive wear and perspiration. This detail brings attention to the strength shown by the woman as she works through difficult conditions to perform her chores for the family. In Supper Time, Pippin simultaneously documented the strength and resilience of African American families while honestly depicting the environments in which they were forced to live. He calls attention to these debilitating disparities that existed throughout his lifetime.10
A Final Self-Portrait?
The Park Bench (1946) was one of Pippin’s last completed paintings (Fig. 4).

Here we see an older black man sitting on a park bench with trees, animals, and natural scenery.11 The painting may have been inspired by Pippin’s observations of a resident who liked to sit at a park near his home in West Chester, Pennsylvania, where he spent most of his life. One might imagine that this painting, done near the end of his life, reflects Pippin himself as the subject. He sits alone on the bench as he thinks about his challenging life, overcoming many struggles through his drive, perseverance, and hard work.
But most of all, Pippin used art as a form of rehabilitation—for the physical and mental-health injuries of war, and as a format/platform to process and work through the social problems of racism and poverty in America. Ultimately, a feeling of tranquility and contentment emanates from this painting, perhaps showing his state of mind toward the end of his life. The Park Bench depicts an elegantly-dressed older man who sits somewhat awkwardly with one arm pushing back on the bench supporting his back and his right leg and foot turned inward in an uncomfortable manner. And yet, he seems fulfilled and at peace in this painting, a final testimony to his faith in art as a tool for rehabilitation and social change.
Although I am a formally-trained developmental biologist and scientific researcher, I am also an avid appreciator, and sometimes practitioner, of visual art. My current work leverages the overlap between science and art to empower trainees from underrepresented backgrounds in their fields. This professional interest grew from my graduate experience where I was continually struck by the similarities between science and art, from process to underlying philosophy. Importantly, the interplay between science and art also deeply impacted my personal rehabilitation from multiple surgeries and injuries during my graduate work. Here I share how art helped me translate a principle from chemistry into a grounding and liberating framework for my own physical healing.[/vc_column_text][vc_empty_space][vc_column_text]
Dynamic Equilibrium in Chemistry, and Beyond?
I was first exposed to Dynamic Equilibrium in a high-school chemistry class, where I learned a definition that didn’t mean that much to me; in college I learned some math to go along with that definition. Dynamic Equilibrium didn’t resonate with me until my graduate elective course in biochemistry, where our professor encouraged us to focus on conceptual implications instead of just solving chemical equations. Professionally, this emphasis on the broad ramifications of biochemistry principles significantly shaped my graduate research. Despite being in a different field, my dissertation focused on how biochemical reactions between just a few proteins can guide an embryo to correctly develop into an adult.1 Personally, it opened the door to applying scientific concepts to my everyday life, something that became profoundly important during my long and tumultuous journey with rehabilitation.
My graduate re-introduction to Dynamic Equilibrium happened 9 months after an unexpected ankle surgery, which was on top of back-to-back knee and Achilles tendon surgeries. My career as an avid soccer player had caught up with me, and I had three major surgeries in as many years. I had just finished my physical therapy regimen, but I was frustrated and confused. I thought finishing my treatment meant I was fully healed, but I felt nowhere close to that! I desperately wanted to feel like myself before the surgeries, but my rehabilitation had been a roller-coaster of breakthroughs and backsteps, peppered with intense frustration and re-injury. Something wasn’t working. Then I was struck by an intriguing overlap with Dynamic Equilibrium: equilibrium is reached when a reaction is ‘done,’ and I desperately wanted to be ‘done’ with my rehabilitation. Perhaps I could find what was holding me back by looking at the process and principles behind Dynamic Equilibrium, gaining clarity from chemistry.
Dynamic Equilibrium Explained
I offer this simple visual introduction to Dynamic Equilibrium and a longer tutorial, both found online. As demonstrated in these videos, in chemical reactions, reactants are converted to products at a certain rate, while products are converted back into reactants at another rate (Fig. 1, left panel). Reactions want to equalize these forward and reverse rates so that there are constant, but not necessarily equal, amounts of reactants and products (Fig. 1, right panel). With constant amounts of reactants and products, there is no visible macroscopic change in the reaction, and equilibrium is reached. Equilibrium is dynamic, however, because individual molecules are still moving through the forward and reverse reactions, just at equal and balanced rates.

What I found remarkable about Dynamic Equilibrium was that even when a reaction is ‘done,’ molecular movement is still happening. This means that the desired end-state in chemistry is one of balanced motion. I wondered if the same could be true for rehabilitation.
But I was stuck; what does balanced motion mean in the context of my physical healing? What does it look and feel like, and how can it be achieved? To tackle these questions, I leaned on my experience with visual art, which had always enabled me to understand complex and nuanced emotions or experiences. By finding examples of Dynamic Equilibrium in art, I hoped to better understand the process and underlying philosophy of balanced motion to inform my rehabilitation.
Translating Dynamic Equilibrium Through Art
In the balanced motion of Dynamic Equilibrium, everything is moving and yet nothing is changing. This dynamism and emphasis on kinetic movement reminded me of the works of Alexander Calder (1898-1976), an American sculptor with a keen and constant interest in depicting motion.2 In fact, Calder redefined sculpture as a dynamic art form since many of his works could actually be in motion,3 as seen here. Perhaps Calder’s most well-known contribution is the mobile: moving sculptures hung from the ceiling with elements or groups of elements that freely and independently move. The mobile’s arrangement is constantly changing as it interacts with its environment, whether by responding to the air currents created by passing visitors or casting a shadow unique to each moment in time.3 A Calder mobile embodies Dynamic Equilibrium because although it is a finished sculpture, it remains in constant motion.
I encountered my first Calder mobile as a child visiting the National Gallery in Washington, DC with my family. Suspended in the quiet and cool atrium of the East Building, the behemoth Untitled revolves slowly (Fig. 2). Designed in 1972 and installed in 1977, the mobile has two main assemblies: the upper section is defined by horizontal wedges, six black and the largest blue, that slice through space, while the lower section is defined by more vertical and triangular panes, painted red, and suggestive of Earth’s gravitational pull. The mobile’s graceful dance on the air currents belies its massive size; with a wingspan of over 85 feet across, the tail misses colliding with the walls by mere inches.4 But, instead of feeling menacing, the mobile feels majestic and even uplifting.

While Untitled epitomizes Calder’s later career, characterized by monumental public works, the Arc of Petals mobile (1941) represents his more intimate works. Arc of Petals is a smaller, vertical cascade just under 8 feet high (Fig. 3). The arrangement feels antigravitational, with larger and far-reaching shapes at the top giving way to smaller, denser, and dangling sections at the bottom5 (Fig. 3). This contrast between the top and bottom assemblies is underscored by color differences: shapes at the top are painted black, while shapes closer to the bottom are shiny, unpainted aluminum. Arc of Petals also hangs lower in its gallery, which, along with its smaller size and vertical arrangement, means that the mobile shares space with the viewer and can rapidly respond to a nearby individual’s movement, as seen here. Uplifting in a different way, this tinkling and twirling mobile invites the viewer to dance, interacting with and transforming art in real time.

Despite these differences, Untitled and Arc of Petals are both intricately-balanced mobiles. Paradoxically, Calder did not achieve this “buoyant” balance2 through perfect symmetry, but through “disparity in form, color, size, weight, [and] motion.”5 Instead of precisely mirroring each other, the varied assemblies of a Calder mobile retain a similar visual weight in direction (vertical or horizontal), color group, or shape, to create a sense of balance.6 This asymmetric balance is as much a hallmark of Calder’s sculptures as their ability to be in motion. Asymmetric balance can also characterize Dynamic Equilibrium since there is a constant, but not necessarily equal, balance of reactants and products.
Dynamic Equilibrium and Rehabilitation
Importantly, Calder’s mobiles revealed what Dynamic Equilibrium could look like: complex assemblies in motion, achieving balance through their asymmetries and constantly interacting with their environment. Even more revelatory was how these visual representations of Dynamic Equilibrium made me feel: both works inspired calm, grace, and ease, reminding me of the beauty of the present moment. They were the embodiment of a deep breath that beckons you to take one, too. This is what I had been missing; I needed to translate how Dynamic Equilibrium looked and felt into my own rehabilitation. I call this mix of capabilities Ease in Motion and I used the process and philosophy behind Calder’s mobiles to guide me to a new rehabilitation framework.
Ease in Motion: A Rehabilitation Framework
If I wanted to achieve the Ease in Motion embodied by Calder’s mobiles, it became clear that the goal of my rehabilitation would have to be different than what it had been. As a competitive soccer player, my goal had solely focused on peak performance; I thought that once I reached a certain level of performance, I would be fully healed. Unfortunately, this level of performance was arbitrary (set more than 10 years ago by this point) and had only led to re-injury. In contrast, Calder’s mobiles were designed for participation: they constantly interact with their environment, from the daily conditions of the gallery to the lived experience of their viewers. Similarly, Dynamic Equilibrium is not a static endpoint, but a constant state of motion. This lens prioritizes the journey over the destination and spurred me to radically redefine what it meant to ‘feel like myself’ again.
From ‘Peak Performance’ to Ease
My goal for rehabilitation shifted from a peak level of performance to an easeful participation in everyday life—but it was not a smooth transition. Without performance metrics to chase, I felt unsettled, disoriented, and uncertain; I needed a framework to ground my focus and measure my progress. Taking direction from Calder’s mobiles, I refined this goal of participation as the ability to adapt and interact with the conditions of the moment. I saw that Calder’s mobiles achieve this through a structural integrity that enables them to remain both in motion and balanced despite asymmetric arrangements. These principles of strength, mobility, and balance became the pillars of my rehabilitation as I sought Ease in Motion.
Achieving Ease in Motion: A Physical Process
How did Calder achieve this strength, mobility, and balance in his mobiles? While other, more contemporary artists have designed mobiles based on mathematical calculations,7-8 Calder’s process was organic and intuitive. He started small, balancing the smallest unit first and then finding a new balance point every time he added a new set of shapes.9 Through this iterative adjustment of each unit or connecting rod, Calder constructed expansive mobiles balanced by their asymmetries.
Importantly, he had to be keenly aware of the asymmetries between shape sets and build sturdy-enough supports to balance the full assemblies. This is where I began: the physical process of assessing my asymmetries and the solidity of my frame.
Finding Asymmetric Balance
My injuries had crisscrossed my body, from left to right then right again. Intellectually I knew I had some imbalances, but it wasn’t until I discovered alignment-based yoga that I physically noticed the prevalence, and sometimes staggering repercussions, of my asymmetries. This awareness enabled me to work with each asymmetry, either as an individual unit or as part of a kinetic chain. I prioritized targeted strength exercises and unilateral movements, and I sought acupuncture, massage therapy, and Graston technique specialists to address scar tissue buildup and nerve pain. I slowly familiarized myself with the tiny and numerous stabilizing muscles of my feet, ankles, knees, and hips, which required a surprising amount of exertion that was often invisible to the eye. Fittingly, this reminded me of the complexity of moving parts in Calder’s mobiles and the vigorous molecular motion of Dynamic Equilibrium.
Adapting and accepting these physical asymmetries (which we all have on some level) also required a closer look at my frame’s foundation: my feet. Surprisingly, as I focused on their strength and balance, my feet expanded, slowly widening until my toes could extend to their full reach and length. To my shock and chagrin, I realized that my shoes (including soccer cleats) were all a half to full size too small! As one would expect, once I gave my feet the space to expand and be fully grounded, I instantly felt more stable and balanced despite my many asymmetries. This podiatric revelation also evoked Calder’s mobiles since, no matter the scale, they fully occupy their space with far-reaching shapes balanced by a sturdy and expansive skeleton.
Achieving Ease in Motion: A New Mindset
Each Calder mobile also has a clear message: slow down and take in the beauty of the world around you.3 This was consistently communicated by invoking nature: the suspended abstract shapes might suggest leaves or petals falling (Figs. 2 and 3) while the unhurried revolutions of each unit mirror the energetic forces that surround us, one of Calder’s core inspirations.2 Importantly, the purpose behind the strength, mobility, and balance in each mobile was to adequately reflect the calm and grace of the natural world. This inspired me to look to nature to contextualize my search for Ease in Motion. What I found was a new mindset for rehabilitation, one that emulates the pace and playfulness of the natural world.
I took Calder’s call to engage with the energetic forces around us seriously and started to garden, hike, and sneak at least a few moments outside each day to connect with my surroundings. I was struck by the gradual yet unfailing change of the seasons (and ability of weeds to grow!); despite moving at a glacial pace, dramatic change could suddenly occur. This mirrored my own experience with rehabilitation, where it often felt like invisible efforts were yielding only miniscule results. And yet, year after year, I could see and feel profound improvement on all fronts. This underscored that nature’s way is not one of static perfection or ‘powering through,’ but instead of accumulating constant, and persistent, small changes. Similarly, Dynamic Equilibrium relies on continuous motion at the molecular level, while Calder’s mobiles coordinate many moving parts to continuously create new configurations.
Finding a Little Fun
Connecting with nature also inspired a child-like wonder10 as I saw that there’s so much to savor when you take the time to look. Calder’s mobiles similarly invite the viewer to step out of the busyness of their daily life and reflect on the joy of being alive.3 Rehabilitation can be a daunting and unfamiliar process, but wonder and play gave me the humility, courage, and patience to persevere or change course when necessary. Although appreciation and humor were essential to my rehabilitation, they were challenging to maintain in the face of traumatic surgeries and daily discomfort. It remains a daily commitment to find something that makes me giggle: a zinger from my favorite tv show, my pet’s bizarre antics, or simply the thought of that colorful and immense arm of Calder’s National Gallery mobile nearly nicking the pristine atrium wall (Fig. 2).
Conclusion
I hope that I have provided a framework that others may apply to their own rehabilitation. Ease in Motion is inspired by the chemistry principles of Dynamic Equilibrium and translated to the human experience through Alexander Calder’s mobiles. Drawing on themes from Calder’s moving sculptures, Ease in Motion encompasses a physical process as well as an underlying philosophy that can be practiced and applied over a lifetime.
I strive for Ease in Motion by embracing asymmetrical balance, expansively taking up space, slowing down to tune in, and encouraging my sense of wonder. This approach to rehabilitation has been liberating, grounding, and, most importantly, effective. I have not only progressed in strength, mobility, and balance, but I am also consistently an active participant in my daily life.
I am deeply grateful for this connection between Dynamic Equilibrium, art, and rehabilitation. It has shown me that I am healed in more ways than I previously thought, and that, paradoxically, the best way to appreciate what I have is to continue my rehabilitation. This continuous tension, or balance, between my desire to move forward and my acceptance that I am perfect as I am is an exhilarating dance of being both healed and healing. Like Calder’s mobile riding the East Building air currents, it is a dance in Dynamic Equilibrium.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Preserving and documenting the lived, pandemic experiences of Pennsylvanians through visual art and creative writing, the Viral Imaginations: COVID-19 project functions as both a historic archive and a reflective, healing resource. Linking the fields of art, health humanities, and bioethics, this interdisciplinary endeavor offers a template for artistic introspection and expression as a method for coping with individual and collective trauma. In so doing, Viral Imaginations overcomes narrative privilege by collecting pandemic stories across diverse intersectionalities.
There is magic in hearing a story and taking what medicine you need from it …
— Maria DeBlassie1
In March 2020, we awoke to the dystopian reality that COVID-19 had become a global pandemic. Our lived experiences had not prepared us for the stresses, strains, and losses of this new reality that began with an extended shelter-in-place phase, which promised—but failed—to curtail the invisible, virulent enemy we did not understand. Life as we knew it dramatically mutated into something unrecognizable and unwelcome—drastically altering how we worked, learned, socialized, provisioned, and grieved.
Yet, despite the shared experience of living under COVID-19, we have each uniquely endured and adapted during days, weeks, months, and now years, as the virus morphs and the pandemic enters new phases. Every pandemic narrative is important, and the telling and witnessing of individual stories serves both therapeutic and humanistic goals of healing and enhancing empathy. The conveying and contextualizing of such narratives are possible through the arts and the humanities, which play varied and important roles in daily life—ranging from expressing shared experiences to contributing meaning to those experiences.2 The arts and the humanities enhance human flourishing;2 part and parcel of human flourishing is the experiencing of wellbeing and the development of compassion for, empathy with, and caring about, others. These goals also reside at the heart of the health humanities, which aid in examining, understanding, coping with, and possibly improving the human condition.
This article details the development of the Viral Imaginations: COVID-19 project, an arts and health humanities endeavor that has attempted to capture vital narratives from across the spectrum of lived experiences during pandemic times. Tackling the exclusionary narrative privilege problem prevalent in the arts, the humanities, and history, Viral Imaginations features creative stories by those traditionally excluded. Moreover, the article provides insights into how similar endeavors would benefit healthcare, including rehabilitation, by creating understanding among and between patients, providers, and others involved in the circle of care.[/vc_column_text][vc_column_text]
Viral Imaginations: COVID-19: History and Purposes
In service to health and humanitarian goals, an interdisciplinary team at The Pennsylvania State University (Penn State) developed the Viral Imaginations: COVID-19 project (viralimaginations.psu.edu). The project strengthened our understanding of pandemic experiences and the ethical issues they raise, as well as established a just-in-time community resource for creatively coping. Launched during April 2020, amid the pandemic’s shelter-in-place phase, Viral Imaginations3 took the form of a publicly-accessible, web-based archive of creative writing and visual art (Fig. 1). To date, Viral Imaginations boasts nearly 350 works by approximately 250 contributors and has attracted more than 15,000 site visits.

Altering Narrative Privilege
Using a health humanities orientation, Viral Imaginations attempted to mitigate the persistent problem of narrative privilege, in which society’s gatekeepers determine what narratives are collected and how they are valued.4 Narrative privilege, or the ability to tell stories through text or pictorial images, has traditionally belonged to the dominant genders, races, ethnicities, and classes, leaving many voices unheard and images unseen. In an effort to minimize gatekeeping, Viral Imaginations gathered creative narratives from Pennsylvanians of all ages, abilities, races, ethnicities, genders, orientations, and locations throughout the state. There are also submissions in a variety of languages other than English, including Spanish and Ukrainian. Maintaining equality across works, submissions were curated into either the visual art or the creative writing gallery by date.
The Artists: Creations From the Heart
Shattering narrative privilege, artist Erika Richards “paints the majesty of Black people penetrating the world…beyond class, race, and culture” as “a reminder…that Black people’s existence surpasses the American History story.”5 In her work, “Pearl Cameo,” in the Viral Imaginations archive, Richards6 depicted a woman within an oval brooch (Fig. 2). Richards created this watercolor as a distraction while recovering from COVID-19 and simultaneously caring for her mother, who was also ill with the virus. Richards explained that as her mother’s illness worsened, she needed to create art to take up “space in [her] head so that [she] would not think worrisome thoughts.”6 Richards described the experience of shedding tears while painting and expressed relief that they did not ruin her watercolor.

In response to the Black Lives Matter (BLM) protests in the summer of 2020, many submitters addressed racial injustice, documenting travesties such as George Floyd’s murder by police. Through their visual reflections, they noted social divisions, highlighting exacerbated racial tensions alongside the pandemic. Calling for connectivity and racial healing, Jenna Deal’s (2021) sculpture,7 “Things We Take for Granted,” featured hugging black and white figures, stressing the importance of the BLM movement (Fig. 3).

Challenging the Art Historical Canon: Outsider Art
Based on elite group preferences, art and cultural canons often reflect the vision of scholars and critics who “embrace” and subsequently “deify” specific artworks.8(p1) The National Gallery of Art defines the art historical canon as a “conventional timeline of artists who are sometimes considered as ‘Old Masters’ or ‘Great Artists.’”9 According to aesthetic philosopher Paul Crowther, “art and the aesthetic are concepts of [W]estern origin.”10 (p55) Although the arts are clearly not exclusive to the West, scholars have traditionally evaluated art forms based on deeply rooted Euro-centric ideologies of worth and value. The vast majority of work within the artistic canon excludes creations by “women,” “non-[W]estern racial groups,” and non-heterosexual individuals, who represent the marginalized and have, as a result, frequently been denied entry to the canon.10 (p58)
Although “canon-making,” according to culture critic Wesley Morris, is an innately human desire, it faces push-back when confronted by the reality of lived experiences that differ from canonical representations.8(p1) Thus, historians look to outsider artists, unburdened by the constraints of the high-art world, for documentation of experiences outside the hegemony. “Disenfranchised from the art world,”11(p250) outsider artists can challenge high culture in ways that those from within frequently cannot. For example, the bold and visually striking work of artist Keith Haring12 exemplifies an outsider narrative of marginalized personal experience—that of a gay, HIV-positive man—to illuminate the lived realities of the American AIDS epidemic during the 1980s and 1990s. Haring provided others with an opportunity to witness his reality through bold colors, basic figures, and clearly communicated messages. Particularly, Haring’s work brought attention to HIV/AIDS and homosexuality in an era of public fear and HIV/AIDS stigmatization.13
Collecting and archiving artworks by diverse creators, many of whom are art-community outsiders, Viral Imaginations preserves authentic memories and concurrent feelings of living though the COVID-19 pandemic. Like Haring’s work, the pieces in the archive provide access to experiences that often occurred below the radar of the public eye, offering a robust perspective of life during pandemic times.
An At-Home Perspective
Created while she was in second grade, virtual learner Zoya Baloch’s “Fun Home,”14 provides a child’s perspective of pandemic life, amid the dysregulation of routines like in-person education and playdates (Fig. 4). While many parents endured stress and anxiety during the pandemic due to juggling working from home alongside their children’s remote schooling, Baloch’s mixed-media map of her home is joyful and refreshing. “I used bright colors because it reminds me of a rainbow,” explained Baloch.14 Chaotic and disjointed, the artwork utilized multiple perspectives. Baloch described her imaginary home as “a little more creative” than her actual home, depicting haphazard sleeping arrangements and a rooftop shower.14

Narrative Ethics: Making History One Story at a Time
The human endeavor of expressing our experiences and engaging with the experiences of others often takes the form of storytelling. Stories convey factual information and emotional content within a context-rich, narrative structure that allows for both self-understanding and meaningful knowledge-sharing.15 “Narratives are interpretive practices through which we make sense of our lives, and these meaning-making practices are ethically charged.”16(p3) Narratives uncover critical ethical insights that cultivate:
“…the key to a self-examined, responsible life; …an ethical relationship to the other; …a means of sharing experiences in ways that contribute to a sense of connection and community; …[the] develop[ment of] capacity for empathetic perspective-taking; and …a form of moral education [that] cultivates our moral powers.”16(p90)
As such, narratives play a crucial role in the arts, the humanities, and bioethics. Specifically, narrative ethics—while claiming no unified methodology—involves the sharing, witnessing, and examination of an individual’s identity-based, lived experiences.17 The purpose of this undertaking is to create an inclusive moral discourse in which voice, perspective, positionality, and personal background matter.17 The uniqueness of the teller’s story and the way it is told, including the language used, carry weight equal to what is told.18 Such narratives may be captured via numerous media, including creative writing and visual art, as in the Viral Imaginations archive.
Creative Writings, Tough Times
On par with Viral Imaginations’ visual art narratives, the archived creative writings capture personal stories from difficult times. David Martin’s19 poem, “Pandemic: Year Two,” shared both factual information about the pandemic and emotional reactions to it, while exploring community, divergent perspectives, and determining what conduct is ethically called for under the circumstances. He wrote:
I thought it would be done by now.
History and scientific wisdom belied my hopes
But I wanted to believe.
Surely we would mask.
Surely we would stay apart.
Surely we would listen.
Friends argued against shutdowns.
(They still do.)
People who’d never heard of hydroxychloroquine
Knew it would turn the tide.
It didn’t.
Half a million Americans aren’t wrong.
As they lie in judgment of those still living.
And here we are
Some of us still masked
Some of us still separate
Some of us listening
Some of us vaccinated
But none of us free
As a second year begins.19
Magnifying the value of such individual narratives, Viral Imaginations also features ekphrastic dialogues between submissions, as submitters found resonance in each other’s stories. Liv Taylor20 connected with Allie Lunger’s21 pencil drawing of a fractured face reflected in a cracked mirror (Fig. 5).

Taylor wrote and submitted the following poetic narrative, “A Response to Allie Lunger’s Many Faces of Mental Health”:
I just don’t recognize her anymore.
She’s right there. Right in front of me.
But the longer I stare, the more I see a stranger. And it scares me. I can feel it in my stomach. Is that what I feel in my veins? Racing through my body?
She’s nostalgic. A stranger I know too well. But no one knows her like I do. Her strengths, her flaws, her habits. No one knows. But me. She’s a stranger, but she’s my best friend.
People think cracks are messy, but she knows better. I know better. Scars are not wounds; they are roots and proof of trials and tribulations. Flowers grow from dirt, so why can’t I? I love my roots. Cracks and all. So why do they scare me?
I know why. Too many cracks, and a mirror breaks. Good thing it’s just a reflection. Because the cracks in my body, in my roots, they’re not glass, they’re roots, and if we know anything about the earth, it’s that roots are strong, and grow from dirt, just like me.
And what’s more beautiful than that?20
Indeed, living in pandemic times has left cracks in our mental health, our routines, and our entire way of being in the world. Capturing the spirit of the Viral Imaginations project, as well as the ethical underpinnings of narrative ethics, Taylor’s20 ekphrastic piece demonstrates how stories told through artistic media help us interpret and embrace our experiences, heal through creative endeavors, and empathetically relate to the plights of others.
Viral Imaginations as Translational Template
The concept underlying the Viral Imaginations gallery and archive could easily translate as a powerful model for healthcare in virtually any specialty. A similar effort could be established either as a publicly-accessible Internet presence, like Viral Imaginations, or as a private intranet platform, featuring artistic expressions by patients, providers, and even nonprofessional caregivers and family members. Such a venue would allow for the sharing of lived experiences addressing illness, disability, recovery, caretaking, and/or loss. Contributions could be cordoned off into galleries dedicated to specific media or separated by contributor identification. As with Viral Imaginations, submissions could include creator name or be anonymized, at the submitter’s option.
Engagement with narratives within contributor-identification groups (ie, patient, caregiver, provider, etc.) would establish a semblance of community, providing patients and their loved ones with a sense of solidarity during arduous, and often confusing, times. Perhaps, even more importantly, engagement with creative narratives across contributor-identification groups could enhance understanding, empathy, and co-created problem-solving by better equipping all parties, especially patients and providers, to engage in more productive ways.
Moreover, a Viral Imaginations-like project could serve as an effective teaching tool for understanding the patient experience and developing enhanced empathy. “[C]ombining narrative pedagogical techniques and visual art can be applied to …diseases, conditions, and epidemics and has been employed in instruction in health care.”22(p 12),23 Creative works can be used to aid health-profession students in recognizing that illness, disease, and disability are as much sociocultural issues as they are medical concerns.22 In similar ways, Viral Imaginations has served as a hands-on learning laboratory steeped in the health humanities for Penn State students across numerous disciplines.
Conclusion
The Viral Imaginations project provided Pennsylvanians with a creative outlet for sharing their pandemic experiences and developing a sense of community. By offering this resource the project brought to life the value of the arts and the humanities in critically addressing crises. Functioning as a creative archive of first-person narratives across diverse intersectionalities, Viral Imaginations preserves for future study self-represented stories of life in pandemic times. Additionally, Viral Imaginations offers up a robust and easily transferrable platform applicable to numerous topical applications within—and beyond—healthcare.
The authors extend gratitude to Viral Imaginations: COVID-19 intern Grace Joseph for her research assistance.


This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Training guidelines for rehabilitation disciplines are generally based on medical models that focus on acquisition of knowledge (eg, anatomy, diagnoses, policies) and skills (eg, discipline-specific interventions) related to different disability diagnoses. However, there are mounting calls to expand the sensitivity of rehabilitation professionals to the personal experiences of, and social biases toward, individuals with disabilities (ie, issues of ‘attitude’). It is argued that the review of artistic depictions of disability in their respective historical contexts offers an excellent vehicle by which to sensitize rehabilitation professionals to these issues. This article reviews the manner in which different western societies throughout history have depicted individuals with physical, mental, and sensory disabilities in the visual arts, ranging from primarily negative (eg, reflection of divine punishment for deserved transgressions, objects to be ridiculed for entertainment, etc.) to more recent positive perceptions (eg, heroes in contemporary films). Suggestions are offered regarding the use of the visual arts to educate rehabilitation professionals regarding individual and societal biases of disability, and to reduce the perpetuation of the stigma, misrepresentation, and mistreatment of individuals with disabilities.
Introduction
Since the passage of the Americans with Disabilities Act (ADA, 1990) there has been increased interest in promoting a better understanding and acceptance of persons with disabilities, as well as improving the societal discrimination they face. The Disability Rights Movement developed primarily in the last quarter of the 20th century with considerable growth in advocacy efforts over the past three decades (eg, see Lives Worth Living). Of primary importance, the ADA prohibits discrimination and ensures equal opportunity for persons with disabilities in: employment; state and local government programs and services; access to places of public accommodation such as business, transportation, and non-profit service providers; and telecommunications. Although the ADA has provided greater opportunities and access for persons with disabilities, in order for them to attain complete inclusion into society, it is essential to change the negative attitudes and misperceptions regarding them commonly held by the general public—as well as by many rehabilitation professionals.
The manner in which individuals with disabilities were perceived, treated, and integrated into societies throughout history is complex and related to multiple issues involving economic, scientific, and religious factors.1 In the past, individuals with disabilities were frequently viewed as objects to be ridiculed and for the most part they have been perceived as a burden to others and considered to be of limited value to society.2,3 This was due in large part to the limited understanding of human anatomy and physiology, as well as the lack of methods to treat disease and injuries, minimize impairments, or develop assistive devices (eg, prosthetic devices, assistive technologies, environmental accommodations). As such, they were often socially ostracized and driven to live on the margins of society. In contrast, there have also been various cultures and religious sects throughout history that have tended to care for and be empathetic toward individuals with disabilities.
Imagery From Ancient Times to the Present Day
Ancient writings and images reveal a wide variety of messages about how individuals with disabilities were treated and perceived in early historical times, including the portrayal of disability as a source of punishment in the Code of Hammurabi (ca. 1780 BCE), as predictors of good or bad events in The Omen Series Summa Izbu (ca. 1300 BCE), as individuals capable of community leadership in Homeric writings (The Iliad, 750 BCE), or even as a mark of beneficence in ancient Egypt.2,4 However, few know that Aristotle proposed a law to prevent parents from raising deformed children,5 that Spartan laws obliged parents to abandon deformed children,6 or that Cicero claimed that the body determined the ‘shape’ of the soul.7 Even numerous biblical passages demonstrate how individuals with various physical disabilities (eg, leprosy and paralysis) were perceived and treated negatively.2,8 In fact, numerous laws/policies throughout history legalized or encouraged discrimination against individuals with disabilities and such negative representations further reinforced public perception of disability as ‘abnormal,’ along with the social division between the disabled and nondisabled.9 These negative perceptions of disability generally persisted until the second half of the 20th century when advances in medicine and innovative treatments/technologies allowed for the approach to disabilities to be improved.
Training in Disability Issues Across Rehabilitation Professions
With the development of the profession of physical medicine and rehabilitation following World War II, society began to view more consistently individuals with disabilities as worthy of treatment, and to assist them in recovering as fully as possible and returning to productive, independent lives.10 Since then, rehabilitation disciplines have developed training guidelines to improve the health and functioning of individuals with disabilities (Table 1). In general, these professional organizations call for training based on medical models that emphasize knowledge and skills, often leading to the treatment of individuals as ‘disorders’ (eg, a spinal cord injury, a traumatic brain injury, a stroke) or ‘impairments’ (eg, forgetfulness, irritability, spasticity), rather than individuals with disabilities. As such, rehabilitation ‘success’ could be over-simplistically evaluated in terms of improvements in range of motion, memory scores, or increased psychological traits, without consideration of the need for full inclusion of individuals with disabilities into society. Because of these factors, it has been concluded that rehabilitation professionals “are often negative about disability, seeing inability before ability and frustrated by the lack of a prospect of cure and ill-informed about simple accommodations.”11(p462)
_______________
Table 1: Rehabilitation Discipline Training Guidelines
American Board of Internal Medicine (2013). Internal medicine/physical medicine and rehab policies. Accessed online on 7/20/2020 at: http://www.abim.org/certification/policies/combinedim/comrehab.aspx
Accreditation Content for Occupational Therapy Education (2018). Standards of practice for occupational therapy. Accessed online on 7/20/2020 at: https://acoteonline.org/wp-content/uploads/2020/07/2018-ACOTE-Standards.pdf
American Physical Therapy Association (2018). Standards of practice for physical therapy. Accessed online on 7/20/20 at: http://www.apta.org/uploadedFiles/APTAorg/AboutUs/Policies/HOD/Practice/standards.pdf.
American Speech-Language-Hearing Association. (2020). Scope of practice in speech
language pathology [Scope of Practice]. Accessed online on 7/20/20 at: https://www.asha.org/certification/2020-slp-certification-standards/.
American Psychological Association Rehabilitation Psychology Division (2012). Guidelines for postdoctoral training in rehabilitation psychology. Accessed online on 7/20/20 at: https://www.apa.org/pubs/journals/features/rep-a0030774.pdf.
American Therapeutic Recreation Association Standards of Practice. Accessed online on 7/20/20 at: https://www.atra-online.com/page/SOP.
_______________
More recently, there has been increased recognition of the need for training in the ability to understand the personal experiences of persons with disabilities and the societal biases experienced by these individuals (sometimes referred to as training in issues of attitude). It is relatively easy to teach knowledge (eg, facts, diagnostic criteria) and skills (eg, procedures, tests, discipline-specific therapies), as these are generally fact-based and able to be memorized. However, it is much more difficult to mold individual and societal attitudes (ie, conscious and unconscious biases and beliefs) about disabilities. Changing attitudes and beliefs, however, is central to improving the lives of people with disabilities given that prejudicial and exclusionary social practices are believed to be greater barriers to social participation than specific mental, physical, or sensory impairments.12 It is important for healthcare professionals to examine their own beliefs about disability and awareness of how persons with disabilities are perceived, portrayed, and treated today, and particularly for those rehabilitation professionals who work with these populations on a daily basis.
Rehabilitation Psychology Training Guidelines: An Example
Although all rehabilitation training guidelines generally focus on the medical model, initial post-doctoral training guidelines for rehabilitation psychology provide an example of training methods to address issues of attitude. This specifically involves the need to be educated about the manner by which disability is a socially-constructed phenomenon, as well as the manner by which our own biases affect our treatment, interactions with, and expectations for, individuals with disabilities. For example, one of the most notable rehabilitation psychology guidelines calls for training in “cognitive, affective, and societal sources of handicapped myths about disability and ways to counteract them.”13 This suggestion is truly unique among the various rehabilitation disciplines in that it acknowledges the significant role that societal expectations and misperceptions have in the manner by which individuals with disabilities are treated. Although this suggestion is noteworthy, there are no specific methods to suggest how to train rehabilitation professionals regarding the societal perceptions that impact persons with disabilities. This article suggests that studying images of disability in art history is an important and impactful method for teaching rehabilitation professionals about the experiences and biases experienced by those patients they serve.
Art as a Means to Better Understand the Experience of Disability
Human beings have made art to communicate and connect with each other since prehistoric times. Art has the powerful ability to help viewers relate to the individuals depicted in the image on a human, empathetic level, which, in turn enhances the goal of understanding and acceptance on a new level. Artists have used various mediums (eg, paintings, poetry, narratives, sculpture, film, etc.) to express emotional turmoil, tragedy, social isolation, and psychological disturbance as a means to relate and share personal experiences. The medical, legal, and social zeitgeist of an era is often reflected by the artwork created of that time. Alternatively, societal perceptions have long been influenced by how individuals with disability are represented to the public visually and politically. There are few primary sources from ancient and medieval times regarding people with disabilities,3 and as a result, researchers have relied on the arts to determine the social context of disability at various times throughout history. In fact, a historian of disability states that, “Studying the representation of disability in literature and art is an important and relatively unexplored research frontier in disability studies.”14(p 54)
The arts have been used in rehabilitation for people with disabilities primarily through recreational therapies in which individuals engage in the visual arts, music, dance, and expressive writing to adjust to their disabilities. However, a review of artistic representations of disability throughout history also offers an excellent method by which to improve the training of rehabilitation professionals. There is increased recognition that studying the humanities helps health professionals gain a better understanding of the human side of chronic disabilities.
People with disabilities are depicted throughout art history, and these images provide a context for the manner by which they were perceived at that time (eg, worthy of derision or sympathy, objects of ridicule, deserving of divine punishment, etc.). For example, prior to the advent of the printing press, when much of the population was illiterate, paintings were often used to tell stories, depict historical events, and provided examples of how people were treated.3 As such, many individuals learned social expectations for how to treat the disabled by viewing paintings in churches or watching plays during community festivals. It is from these works of art that we can understand the culture of the times and become sensitized to the relevant social issues of the day as they pertain to disability. By comparing past and current art forms (eg, paintings, drawing, and sculptures from the past to movies, films, and literature from the present) it is possible to better understand how societal perceptions have a major influence on the way individuals with disabilities are treated. Subsequently, training methods can be developed to counter “social myths of disabilities” (see APA Division 22 training guidelines), and educate rehabilitation professionals to become better providers for individuals with disabilities.
PART 1: The Representation of Physical Disability in Art History
Throughout history, individuals with physical disabilities have primarily been perceived and represented as ’misfits, fools, oddities, and marvels,’ present in the world for purposes of entertainment, ridicule, and experimentation.2 This relates in part to the lack of understanding of the causes of physical disability, as well as the lack of resources, knowledge, or will to develop accommodations during various historical times. As such, individuals with disabilities often had little support from their families and communities and needed to fend for themselves in creative ways; this was generally the case until the last half of the 20th century.
As an example, Greuze’s The Paralytic (1763; Fig. 1) is one of the few depictions of an individual with paralysis, likely due to the fact that the survival rates for such individuals were extremely low.
_______________

_______________
Historically, depictions of physical disability in western civilizations have largely focused on ‘abnormalities’ and the negative manner by which individuals with disabilities were perceived and treated. In fact, a frequently-cited theory from the late 18th century related to physiognomy concluded that the disabled were, “[t]he morally worst, the most deformed.”15 However, it is noteworthy that ancient Egyptian and Greek cultures at various times were generally accepting of individuals with physical disabilities, as illustrated in several of their works of art.4,16,17 For example, a stone carving from approximately 1300 BCE shows a realistic depiction of an Egyptian leader with a withered leg, apparently from polio (Fig. 2). Greek vases show similar representations of dwarves who were valued as assistants within the medical field, and even portrayed as deities.16,17 However, throughout history, such positive depictions of physical disabilities were the exception rather than the rule.
_______________

_______________
By the Middle Ages, societies began to extend to people with impairments “an acceptance at times awkward, at times brutal, at times compassionate, a kind of indifferent, fatalistic integrations” to people with impairments. 8(p15) However, in general, individuals with disabilities were represented as abnormal, with early portrayals exploiting these abnormalities for amusement. Paintings from this time indicate that individuals with disabilities were viewed in terms of a religious model of disability, in that individuals were believed to be disabled secondary to spiritual transgressions and were thus treated with religious interventions, if they were even treated. Metzler2(p89) reports “anecdotal evidence suggests that there was a very strong feeling that malformed babies indicated sin on the part of their parents.” Spiritual interventions for disabilities were depicted in a painting by di Benvenuto (15th Century), titled St. Catherine of Siena Exorcising a Possessed Woman (Fig. 3), in which individuals with both physical (ie, characters with crutches) and mental illnesses (central figure) caused by demonic possession were treated with religious interventions within a church setting.
_______________

_______________
By the 16th century, the Renaissance began to focus on classical forms of beauty, which did not typically include the disabled or deformed. However, art from the northern Renaissance depicted individuals with physical disabilities in a realistic manner, providing insight into the way they were treated and socially perceived at that time. Hieronymous Bosch painted a series of 31 ’cripples’ in 1500, illustrating the various disabling conditions and prosthetic devices used by these individuals.19 Similarly, Bruegel’s The Cripples (1568; Fig. 4) shows individuals with various prosthetics gathered together in a town square. However, historical context indicates that these individuals were forced to wear fox tails attached to their clothes as indicators that they were objects to be ridiculed at community festivals.19,20 Similarly, Bruegel’s Battle Between Carnival and Lent (1559; Fig. 5) shows the relative isolation faced by individuals with disabilities within their communities. Compared to the so-called ‘normal’ citizens participating in either carnival or lent, details from the painting show two groups of individuals with disabilities (ie, ‘cripples’ in middle scene, blind individuals by church entrance) as socially-isolated beggars. These community spectacles are precursors to the freak shows that gained popularity in the mid-16th century and lasted to the mid-20th century, which displayed physically unusual or deformed humans for a source of entertainment21 (Fig. 6). By the 19th century, individuals with impairments were even criminalized through public policy (ie, ’ugly laws’ involving social restrictions placed on those with physical appearances that might offend ’normal’ people)9.
_______________



_______________
Paintings such as Wyeth’s Christina’s World (1948) provide an example of the social isolation and handicaps faced by many individuals with physical disability even in the middle of the 20th century. This painting appears to show its subject, Christina Olson, admiring a homestead in a windswept field. However, an article in the Journal of Child Neurology22 indicates that Wyeth was portraying a young woman suffering from a progressive neurological disorder that he observed crawling crab-like up to her farmhouse. This knowledge challenges the initial perception of the scene and shifts our position from viewer to Christina’s own perspective. This is the power of studying art history: to guide the viewer by facilitating close looking, deeper contextual understanding, and empathy. An article by J.O. Ballard in JHR is an excellent resource for those who would like to use this painting to increase clinical observation and diagnostic skills regarding disability in health sciences education.23
Even within the past quarter century, controversy surrounding the Franklin D. Roosevelt (FDR) Memorial in Washington, DC illustrates the current difficulties society has in accepting individuals with physical disabilities. FDR’s Splendid Deception24 recounts how the original statue of FDR to be placed at the front of his memorial in Washington, DC was designed to depict him in his wheelchair (he could not walk after contracting polio at age 39). However, when the original sculpture was finished, his cape covered his wheelchair completely, in effect hiding his disability (Fig. 7). A second statue, depicting FDR using his actual wheelchair and placed at the other end of the memorial, was completed only after significant advocacy efforts by disability rights groups. It is important to note that ancient Egyptian society could realistically portray important figures with disabilities with compensatory devices over 3,000 years ago (Fig. 2), but the FDR Memorial planners of the 20th century had problems acknowledging his disability, despite the fact that he was one of the most important and powerful leaders in the world during his lifetime.
_______________

_______________
PART 2: The Representation of Mental and Intellectual Disability in Art History
Up until the 19th century, individuals with physiologically-based mental disorders were conceptualized in terms of ‘madness’ primarily related to spiritual disorders that needed to be treated through spiritual interventions (although these beliefs persist in some communities even today). For example, di Benvenuto’s St. Catherine Exorcising a Possessed Woman, shows a demon being exorcised from a woman’s head in the 1300s (Fig. 3). Similarly, Droeschout’s To this Grave Doctor Millions do Resort from the 17th century (Fig. 8) shows a scene in which demons were exorcised from an individual’s head in a fancy contraption (figure on right), as well as from their bowels by the apparent use of an elixir to dispel demons (figure on left).
Similarly, a 16th-century painting by Hieronymus Bosch titled The Extraction of the Stone of Madness (Stones of Folly) illustrates the belief at that time that ‘madness’ was due to the presence of a stone within the skull that required extraction in order for the person to be cured (Fig. 9). By 1514, mental illness was believed to be related to an imbalance of the four humors of the body (black bile, yellow bile, blood, phlegm) that led to the four primary human temperaments (melancholic, phlegmatic, choleric, and sanguine)25 as represented in Durer’s Melancholia I (Fig. 10). Frans Hal’s Malle Babbe (1633-1635) illustrates how mental illness (eg, insanity, alcoholism) was conceptualized in northern Europe during the 17th century as being caused by the visitation of the bird of lunacy (Fig. 11).
_______________



_______________
Art from the 19th century demonstrates how mental (ie, lunacy) and developmental disabilities (ie, ‘idiocy’) started to be conceptualized in a different manner in some cultures, in that such disorders were transformed from being conceptualized as ’madness’ to ’mental illness’ (ie, a medical abnormality)26. For example, in the 1800s, health professionals attempted to distinguish between different types of mental disorders through the identification of unique facial features, similar to the field of physiognomy.
Theodore Gericault painted a series of 10 ’portraits of the insane’ (The Madwoman, 1819-1822; Fig. 12) depicting physical attributes that were thought to be associated with specific psychological disorders—five of the paintings which still exist (Woman Addicted to Gambling, A Child Snatcher, Woman Suffering from Obsessive Envy, Kleptomaniac, Man Suffering from Delusions of Military Command). Although it is difficult to determine how physical features could reveal a ’child snatcher’ or someone with ’military delusions,’ it is noteworthy that mental illnesses were starting to be categorized in terms of specific abnormalities (ie, physical and psychological).
_______________

_______________
Art from other historical periods also offers insight into the manner by which individuals with mental disabilities were segregated and isolated from their communities. Bosch’s Ship of Fools (1490-1500; Fig. 13) depicts the practice during the 15th century and beyond of rounding up the disabled and unwanted and placing them in a wagon with promises of goods, in order to remove them from society.27 This practice changed in the beginning of the 18th century when individuals with mental and sensory disabilities began to be institutionalized in hospitals or asylums, but without prescribed care or interventions.2,3 Goya illustrated such a lunatic asylum in the 1700s (Fig. 14), but incredibly, this representation differs little from the demeaning conditions depicted in the infamous 1970s documentary about the Willowbrook Mental Institution in New Jersey (Fig. 15). These works of art show how individuals with mental illnesses from the Middle Ages until the 1970s were removed from society and deemed unworthy of treatment, which differs considerably from current societal understanding and increasing acceptance of mental illness.
_______________



_______________
Although artists throughout history have generally depicted individuals with intellectual disabilities in a negative manner (eg, village idiots, fools), several works of art illustrate how some societies had positive and accepting views of individuals with intellectual disabilities. For example, The Adoration of the Christ Child (circa 1515) offers a powerful message about the acceptance of individuals with developmental disabilities in Northern Europe in the 16th century (Fig. 16). In this painting, medical professionals have suggested that two of the angels surrounding the manger have Down’s syndrome (although the syndrome was not known as such at that time).28,29 This painting likely reflects the longstanding and continued willingness of communities in northern Europe to be inclusive of individuals with intellectual disabilities.
_______________


_______________
PART 3: The Representation of Sensory Disability in Art History
Misperceptions and prevailing attitudes of individuals with sensory disorders date back to the biblical era. In its most dramatic fashion, select scriptures led many to believe that God used deafness and blindness as retribution for sin: “Who gave man his mouth? Who makes him deaf or mute? Who gives him sight or makes him blind? Is it not I, the Lord?” (Exodus 4:11); “…if you do not carefully follow His commands and decrees…all these curses will come upon you and overtake you: the Lord will afflict you with madness, blindness, and confusion of the mind. At midday, you will grope around like a blind man in the dark.” (Deuteronomy 28:15). This demonization of the blind carried on through the Middle Ages and into the Renaissance.
For example, a manuscript from the 14th century, The Romance of Alexander,30 includes illustrations, in the margins, of the daily customs, work, dress, leisure activities, and social norms that existed in Medieval Europe at that time. Of interest, one border illustration shows how individuals with visual impairments were paraded before communities as a form of entertainment at times of festival (Fig. 17), similar to Bruegel’s The Cripples (Fig. 4). Writings from 1425 describe a similar event:
“Note, the last Sunday of the month of August there took place an amusement at the residence called d’Arminac in the Rue Saint Honore, in which four blind people, all armed, each with a stick, were put in a park, and in that location there was a strong pig that they could have if they killed it….and there was a very strange battle, because they gave themselves so many great blows with those sticks that it went worse for them, because when the stronger ones believed that they hit the pig, they hit each other, and if they had really been armed, they would have killed each other. Note, the Saturday evening before the aforementioned Sunday, the said blind people were led through Paris all armed, a large banner in front, where there was a pig portrayed, and in front of them a man playing a bass drum” (as cited in Wheatley26( p1)).
_______________

_______________
Throughout history, images of the blind beggar have rendered public perception of blind individuals as helpless, useless, and passively dependent. Given the social, vocational, and financial difficulties associated with blindness and marginalization, some blind individuals have succumbed to accepting this role. For example, Millais (1856) portrayed a young blind girl relegated to beg for money by playing her concertina while wearing a sign on her neck displaying the words, “Pity the Blind” (Fig. 18). This was also depicted in a notorious photograph by Strand in 1916 of an impoverished blind woman in New York City, identifying her disability with a sign around her neck saying “Blind,” below the metallic license she needed to obtain to legally beg31 (Fig. 19).
_______________


_______________
Beginning in the 17th century, the perception of individuals with visual disabilities as defective, expendable, and intellectually disabled led to the social control movement of institutionalization for the disabled. In fact, one of the first institutions for disabled individuals was intended for the deaf and the blind, as depicted in Goya’s Yard with Madmen (1794; Fig. 14), which represented scenes of institutions he personally witnessed, and was said to be painted at a time when he feared similar consequences from his own mental illness and deafness. The emotional toll of the blind and deaf, due to marginalization and social stigma, can also be seen in Goya’s Two Old Men (from his Black Painting series; Fig. 20), capturing the darkness and isolation felt during his years plagued with deafness and physical ailment. Similar sentiments are aroused in Degas’ Madame René de Gas (1872/1873; https://www.nga.gov/collection/art-object-page.46599.html), a portrait of his blind sister-in-law’s vacant gaze representing her solitude and isolation, and Picasso’s The Old Guitarist (1903), both depicting tones of sorrow and loneliness. The sorrow and frustration were a product of living in a society that deemed them incapable and blemished, therefore discounting their intact capabilities that could benefit from accommodation.
_______________

______________
During the mid-20th century, Americans with visual impairments described the impact of the beliefs, superstitions, and the social/physical environment as the primary obstacle to the emotional and physical adjustment to their disability, as cited in The War Blind in American Social Structure:
“All too frequently the great tragedy of a blind person’s life is not primarily his blindness, but the reactions of the family and social group toward him as a non-typical member.”32
Today, while ambiguous perceptions of those with sensory impairment still exist, knowledge, technological innovation and accommodations leading to expansive and ready access of support helps afford these individuals education and greater independence. Interpreters are more readily available in health care and educational facilities, along with the transcription of texts to Braille or auditory recordings. With these supports and greater public knowledge, individuals with sensory disabilities have disproved past perceptions of being passive, dependent, helpless, unproductive, or intellectually disadvantaged.
PART 4: Modern Artistic Representations of Disability
Although beyond the scope of this article, it is noteworthy how primary art forms of today (ie, movies, TV) have played a substantial role throughout the 20th and 21st centuries in shaping societal attitudes toward disability. Thus, it is not surprising that the manner by which disability is represented in media art today has also led to greater acceptance of disability. Such realistic and positive representations of disability will continue to teach people who are secure in their beliefs and perceptions of ‘normalcy’ that individuals with disabilities are not subjects to be gawked at or marginalized.
For example, children today are exposed to positive images of disability and representations of characters with disability as leaders, such as those portrayed in the Disney movie Finding Nemo (2003). X-Men is a popular comic magazine that has been made into a series of movies (2000-2019). Of note, Charles Xavier, the leader of this band of individuals with superhuman powers, is confined to a wheelchair. Similarly, the critically acclaimed Murderball (2005) is a documentary film that shows individuals with various forms of paralysis engaging in full-contact rugby in the Paralympic Games in Athens, Greece.
The depiction of mental illness in film has also improved over the past 50 years, with individuals with mental illnesses and sensory disabilities portrayed more realistically and empathetically (One Flew over the Cuckoo’s Nest (1975); Rain Man (1988); Children of a Lesser God (1986)). Rehabilitation trainees and professionals can watch these and other movies that show the human experience of disability with subsequent discussion at scheduled training opportunities (Table 2). These movies offer opportunities to discuss differences in how individuals with disabilities have been portrayed and treated in the past and currently, and how more positive portrayals can lead to the development of better skills for rehabilitation professionals—and ultimately greater understanding and acceptance of the personal experience of disability.
PART 5: Disability Training Through the Arts
It is suggested that rehabilitation training guidelines promote opportunities for both students and professionals to become aware of the “cognitive, affective, and societal sources of handicapped myths about disability and ways to counteract them” (see APA Division 22 training guidelines) through the study of disability in the visual arts. It is recommended that rehabilitation students and professionals review and discuss the visual arts (and literature) relating to the personal experiences of, and societal perceptions of, disability in existing didactics, grand rounds, and journal clubs. Students and professionals can easily review paintings and articles presented in this article for discussion, and particularly those presented in articles from traditional medical journals and art history journals and textbooks (see References below).
Training directors can also find appropriate topics and offerings on art and disability through many websites and organizations (Appendix 1). Review of the representation of disability in the visual arts can also be discussed based on academic sources that provide contextually-relevant cultural information related to specific eras, as well as autobiographies, novels, and collections of short stories that provide examples that relate the personal experiences of persons with disabilities, the challenges they have faced, and the successes they have had in becoming full members of society (Appendix 2).
Conclusion
In conclusion, this article reflects the benefits and necessity of training in the health humanities (versus medical humanities) for both rehabilitation professionals and those individuals with disabilities they serve. Specifically, the health humanities apply transdisciplinary practices that draw on the humanities, fine arts, and social sciences to bring meaning to human experiences of health and illness, to increase social justice for individuals with illness and disabilities.34 Training in the health humanities can complement training in the medical humanities—which focus on the use of the humanities in service to medicine—to help practitioners learn attributes such as empathy, communication, and compassion.
The authors wish to acknowledge the assistance of Josiah Scott in editing and formatting this article.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
.jpg){kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The human body is largely the same from one person to the next. Collectively, bones develop to form a skeletal structure absent of subjectivity. Muscles originate from one area of the body and insert onto another, creating a distinct and purposeful path for movement. The circulatory and nervous systems travel like a network of rivers, giving life to our deepest and most hidden structures. The human body is often visualized in this sameness, and anatomy textbooks have defined it from this objective viewpoint for obvious and well-intended purposes.
However, previous theoretical and humanities-driven work tells us that the body as a whole is much more complex and unique.1 Bones, muscles, arteries, veins, and nerves are found in all of us and act as the foundation for where our bodies and our stories begin. However, defying all logic, the human body courses through life resulting in something that is much greater than the sum of its original parts. It becomes a representation of its collective past and individual experiences—a story that requires deeper understanding and cannot be told in the pages of an anatomy textbook.1
Conceptualizing bodies as both collectively the same yet subjectively unique can be challenging. The history of art provides an effective way to explore the objective and subjective description of bodies; analysis of art provides rehabilitation professionals the opportunity to deepen their understanding and insight into the untold stories of their patients.
Understanding that human bodies are more complex than their individual parts teased out in terms of pain, range of motion, and strength during an exam is crucial for a Doctor of Physical Therapy student working with patients. Throughout my education I have sought opportunities that allow me to further explore these theoretical concepts about the body—how it’s perceived, how it’s felt and experienced by the person who inhabits it, and what makes it unique. Taking time to critically examine art from these different perspectives has improved my understanding of the complexities of the human body.
Disability Represented in Art
In Spring 2018, I had the opportunity to participate in a novel pilot program that brought together dancers, art historians, disability studies scholars, educators, and students in an effort to expand the lenses through which art is perceived. Through critical evaluation and historical research of visual artwork, this collaboration aimed to explore how disability is represented in art, challenge traditional perspectives of movement and disability, and spark dialogue about the representation of bodies in art.
Full Radius Dance (FRD), a physically integrated dance company based in Atlanta, Georgia, was the driving force behind this initiative. FRD seeks to re-write the script when it comes to movement, dance, and disability. By merging disabled and non-disabled bodies in their performances, FRD is fundamentally changing the dialogue around and about disabled artists and performers.
This pilot program uniquely blended the visual arts evaluated at the High Museum of Art in Atlanta with the physically-integrated dance performances of FRD. Pieces of visual art, such as those by Jean-Michel Basquiat (1960-1988), were evaluated from a disability studies perspective. FRD used these evaluations to inform choreography performed among the artwork at the museum (Figure 1). Working in synchrony with the visual artworks evaluated, this performance offered an invitation into the disability-experience culture and an opportunity to listen to and engage with the story they were telling.
My experience with this interdisciplinary pilot program serves as the background for the development of this article. Using Basquiat’s artwork as an example to better understand the subjective nature of the body, in concert with the performance by FRD and their commitment to redefining how bodies are represented in art, I aim to explore how the narrative held within our bodies unfolds. Finally, by linking these concepts to my experience as a Doctor of Physical Therapy student, I hope to create meaningful clinical applications for how clinicians can recognize and listen to the untold stories of their patients.
 Figure 1. Three dancers from Full Radius Dance are captured in mid-performance at the High Museum of Art in Atlanta, Georgia. Their arms are outstretched wide and rest on one another, creating a delicate horizontal line connecting their movements. The dancer on the far left is in a wheelchair with the right wheel slightly lifted off the ground, suspending body and metal together in space. The dancer in the middle is half-kneeling, her body weight shifted directionally toward the right, while the dancer on the far right is propped on her right arm with her back toward the camera, her gaze toward the left. Museum visitors walk in the background. This extraordinary moment depicts in real time how movement is a human experience always in flux.
Figure 1. Three dancers from Full Radius Dance are captured in mid-performance at the High Museum of Art in Atlanta, Georgia. Their arms are outstretched wide and rest on one another, creating a delicate horizontal line connecting their movements. The dancer on the far left is in a wheelchair with the right wheel slightly lifted off the ground, suspending body and metal together in space. The dancer in the middle is half-kneeling, her body weight shifted directionally toward the right, while the dancer on the far right is propped on her right arm with her back toward the camera, her gaze toward the left. Museum visitors walk in the background. This extraordinary moment depicts in real time how movement is a human experience always in flux.
The Appeal of Basquiat
When critically evaluating pieces of visual art at the High Museum using a disability studies lens, I quickly realized the value of Basquiat’s work. I discovered how Basquiat skillfully depicts the human body and encapsulates it with symbolism and text to form a type of visual language, telling his story—and that of many others. At its very core, Basquiat’s work awakens the realization that our bodies and the stories they tell are conceived in sameness yet fueled by our personal histories.
Basquiat’s knowledge and use of anatomy have been explored to a great extent in previous literature—specifically, how he embodied his cultural background and experience as a young black artist.2
I have found Basquiat’s art to be significant in the context of pain and disability; his images can be used as powerful tools for rehabilitation professionals seeking insight and perspective into the complex and layered nature of one’s identity. Biological form alone is only one small piece of a person’s story. History, heritage, and experiences all merge together in unity with our anatomical bodies to form a type of hidden and unspoken personal narrative, shaping how we live in and experience the world around us. Basquiat encourages—and at times, forces—viewers to confront the reality of his story while urging us to consider the complexity of our own.
Looking at Basquiat’s paintings can be like looking into an unknown galaxy. There’s a sense of both fear and excitement as you try to make sense of and rationalize the shapes, colors, lines, words, and symbols sprawled across the canvas. This is the backdrop for the visual language and storytelling Basquiat created. Layers of bright color that uninhibitedly fill space, lines with no real origin, symbols and text written down and crossed out, just to be written over again. Basquiat’s art, much like ourselves, is complex and dynamic. Yet, the way he merged text and symbols provides a roadmap of sorts to the story Basquiat is telling about the world around us; they can be important indicators of the lives of the oppressed. Much like Basquiat himself, straddling two distinct worlds—one of fame and fortune and the other of injustice and racism—his art created space for black bodies and black stories during the 1980’s when the art world was dominated by white, upper-class artists.2,3
Basquiat and the Body
The anatomical drawings and references commonly found in Basquiat’s art—and one of the reasons his art is so applicable to rehabilitation professionals—was largely influenced by a gift from his mother.4,5
In the summer of 1968, Basquiat was playing outside his Brooklyn home when he was hit by an oncoming car.5 He survived multiple fractures and internal injuries and was hospitalized for more than a month, enduring multiple surgeries.5,6 During this time, Basquiat’s mother gifted him a Gray’s Anatomy textbook in the hope that it would help him better understand his injuries and what was happening to his body.5,6 This textbook appeared to have a lasting impact on Basquiat’s artistic career, as he frequently depicted both realistic and abstract anatomical drawings that served as integral components of his visual language.3
In homage to the anatomical human body, Basquiat often drew inspiration from the work of Leonardo da Vinci.6,7 Many of Basquiat’s paintings seem to reference Leonardo’s detailed and precise anatomical drawings and appear to provide insight into Basquiat’s knowledge and appreciation of the human form.
Moving beyond his more realistic anatomical drawings, Basquiat began to explore the human body in more loosely defined terms, allowing space for further interpretation of his work. In Back of the Neck (1983), Basquiat continued to portray a fragmented body like those found in his da Vinci-inspired studies; but this time, the margins aren’t quite as clear. Unlike the da Vinci-inspired pieces, the representation of the human body in Back of the Neck is less direct and calls for deeper analysis of the text and symbolism to identify the story Basquiat is trying to tell. The namesake of the piece alone, Back of the Neck, may indicate a type of vulnerability Basquiat feels to the way his story is being told. For example, despite his reputable status in the art world, he remains vulnerable to the injustices often experienced by black men and may fear he will be known more for the color of his skin and not his artistic talents.8 This type of dichotomy plays out in many of Basquiat’s pieces and can be used as a means to explore the multiple perspectives of a person’s story.
In comparison to Basquiat’s more abstract renditions of the human body, FRD takes a similar approach to choreography and dance, often blurring the lines between the expected and unexpected, the disabled and non-disabled, and traditional ideas about movement (Fig. 2, Fig. 3). By featuring physically integrated choreography, FRD is redefining the meaning of movement and highlighting the work and talents of disabled artists. Additionally, the dancers of FRD appear to embrace their experience—and perhaps the vulnerability that comes with it—as disabled individuals and disabled artists. Basquiat’s visual artworks and the FRD performance both work to confront the duality of a lived experience while challenging societal norms about who can create and experience art.
[one_half] Figure 2. The dancers in this image adopt a chaotic vertical formation that captures various forms of movement as some dancers are in wheelchairs and others are not. At the top of the formation is a dancer proudly holding a wheelchair wheel in her right hand, illustrating the deep embodiment of metal and flesh. A group of museum visitors walk up and down the switch-back style ramp in the immediate background. A little boy, almost out of frame, gazes back toward the performers. The multiplicity of movements forms a fluid visual tapestry.
Figure 2. The dancers in this image adopt a chaotic vertical formation that captures various forms of movement as some dancers are in wheelchairs and others are not. At the top of the formation is a dancer proudly holding a wheelchair wheel in her right hand, illustrating the deep embodiment of metal and flesh. A group of museum visitors walk up and down the switch-back style ramp in the immediate background. A little boy, almost out of frame, gazes back toward the performers. The multiplicity of movements forms a fluid visual tapestry.
[/one_half] Figure 3. The dancer in this image adopts a posture that mirrors the 8-foot-tall bronze sculpture, “Minotarus” by Nandipha Mntambo, which stands behind her. The dancer’s wheelchair is tipped forward, her arms are lifted high above her head with her fingertips pointing outward; her gaze is strong and steady toward the ground. Much like the sculpture she stands in front of, the dancer’s pose challenges our understanding of the human form and empowers us all to explore the ambiguous parts of our physical selves.
Figure 3. The dancer in this image adopts a posture that mirrors the 8-foot-tall bronze sculpture, “Minotarus” by Nandipha Mntambo, which stands behind her. The dancer’s wheelchair is tipped forward, her arms are lifted high above her head with her fingertips pointing outward; her gaze is strong and steady toward the ground. Much like the sculpture she stands in front of, the dancer’s pose challenges our understanding of the human form and empowers us all to explore the ambiguous parts of our physical selves.
Clinical Note: Rehabilitation professionals can use these dichotomous narratives to understand how a patient may present objectively strong and healthy, yet under the surface be feeling the exact opposite. Being in tune with the duality of a person’s experience can inform our decision-making process and create new avenues to promote healing.
Basquiat and the Narrative
From an early age, Basquiat used words and phrases just as much as lines and colors to express himself and analyze the world around him. After dropping out of high school at the age of 15 and leaving the comfort of his home for the streets of lower Manhattan, Basquiat quickly learned about the injustices of the world and his place in it as a young black artist.5
Like today’s mysterious Banksy, Basquiat began his prolific career in 1977 anonymously under the pseudonym, SAMO©.3-6,9 Partnering with a friend, Basquiat wrote cryptic and philosophical messages around the city that challenged traditional thought on race and culture. Basquiat was turning the world of graffiti on its head—and people began to notice. The work of SAMO© commanded the attention of both the general public and the New York City art scene to the stark realities of the world around them. Basquiat was an expert at making people comfortably uncomfortable by challenging traditional thinking and bringing context and depth to conversations about race, religion, and culture. The narrative talents of Basquiat, modeled through the work of SAMO©, is an important reminder of how his targeted use of text had the ability to describe deeply-rooted and complex social issues.
Running in a similar vein, performances by FRD work to challenge societal norms about dance, art, and disability. By integrating the metal and carbon fiber frame of a wheelchair into modern dance techniques, FRD is offering an opportunity for us to more deeply consider the meaning of movement and the story that movement tells. With long-established attitudes and beliefs about disability and the societal boundaries that have limited the spaces where people with disabilities can share their story, FRD is creating a path where these narratives can be heard and shared (Fig. 4).

Figure 4. In this image, four dancers form a small, quiet circle, their backs to one another as they face out into the crowd. Their arms are strongly held next to their bodies. The formation showcases the integrated nature of the dancers, two of whom are in wheelchairs while the other two are standing. The stillness of their small circle becomes even more evident as you notice the large crowd of museum visitors forming around them. Many are sitting on the ground and watching, while others pass by without notice – a common experience when living with a disability in a society that often overlooks your capabilities and human connectedness. But this image, frozen in space, surrounded by movement and varying postures, connects all the bodies present in time.
Clinical Note: For students, educators, and clinicians working in the field of rehabilitation, Basquiat’s art and the work of FRD are valuable resources to help us better understand the complexities of the human body, and how our physical bodies hold unique and untold personal narratives. By acknowledging the human experience as it is and listening to these untold stories, rehabilitation clinicians will be better equipped to provide compassionate and healing care.
An Innovative Disability Perspective
Rehabilitation professionals, students, patients, and caregivers who are dedicated to approaching healing from a humanistic perspective must gain a clearer understanding of disability studies. Basquiat’s work and the work of FRD challenges us to open our eyes to the many layers of the objective and subjective body, to consider how identities are formed through a collage of experiences, and to view the body as a piece of that story. Unlike the performances by FRD, Basquiat’s art is not explicitly tied to those with disabilities. The connections, however, remain relevant and, for the most part, are largely untapped within the health humanities literature.
One of Basquiat’s works in particular, Untitled (Cadmium), was evaluated by the FRD program from a disability studies perspective. In the piece, Basquiat surrounds a black male body with strong personal symbolism of his cultural and religious identity.2 The body itself appears to have scars and the face has eyes and a mouth painted white. For me, this piece is indicative of the level of awareness Basquiat had about his own body and story, and the bodies and stories of those who walked before him. It represents Basquiat’s unbridled talent for merging the anatomical body and the narrative body together into one, much like how FRD merges disabled and non-disabled bodies into one beautiful, storied movement.
For rehabilitation professionals, observing the body in its anatomical form is a common practice used to assess, identify, and treat regions of pain or weakness. It is understood, however, that the pain often experienced by patients can be rooted more deeply than in the anatomical structures themselves. It is here where our standard practice of observation becomes more complex, relying on alternative methods to come up with effective solutions for our patients.
Clinical Note: Basquiat’s use of the human body in his art, paired with the way FRD portrays movement, runs parallel to that of how rehabilitation professionals observe the body in practice. Basquiat produces art that skillfully layers both the seen and unseen aspects of the human body, while FRD layers choreographed movements with flesh and metal. When working with patients, there is a layered nature to both pain and disability. These layers tell a story about the body that is unique to the individual and informed by their personal histories and experiences. Through observation and analysis of Basquiat’s work and FRD’s performances, we slowly become awakened to the story being told within our own bodies and the bodies of those around us

![]()
This work is licensed under a Creative Commons Attribution 4.0 International License.
The groundbreaking book Portrait of Spirit: One Story at a Time1 was envisioned and created by award-winning photographer Billy Howard and nationally-renowned folklorist Maggie Holtzberg. It features photographs of 25 individuals alongside their personal and compelling stories that dance around a single shared characteristic: disability.
In the shadow of the 1996 Paralympic Games in Atlanta, GA, Howard and Holtzberg expertly wove their unique talents together to highlight individual stories of people living with disabilities. Published only six years after the Americans with Disabilities Act (ADA) was passed into law, Portrait of Spirit redefined what it meant to be living with a disability, and exposed the many hidden challenges that must be overcome each day to function within society. At such a pivotal time in history, Howard and Holtzberg opened the door to more meaningful dialogue on disability while providing new perspectives on the disability experience. By focusing on all aspects of each person’s unique story, they emphasized how disability represents only a piece of that individual. Featured in the Portrait of Spirit are artists, mothers, fathers, athletes, educators, advocates, and more, whose voices have been shaped from experiences that transcend their physical limitations.
Almost 24 years since being published, in an act of revitalization, the Journal of Humanities in Rehabilitation partnered with Emory University’s School of Medicine to host an exhibit of the images and stories told in Portrait of Spirit: One Story at a Time. The exhibit ran from October 7, 2019 through November 7, 2019 and served as a mechanism for people to pause, engage with, and contemplate stories that were different from their own. On the opening night of the exhibit, Billy Howard and Maggie Holtzberg, along with some of the individuals featured in Portrait of Spirit, reunited and joined the community in a panel discussion.This discussion revealed how these stories have evolved and provided insight into the continued societal challenges of living with a disability.




This article includes excerpts from Portrait of Spirit: One Story at a Time and offers reflections from photographer Billy Howard on the history that informed the development of this project, and on his personal motivation and experience working with people living with disabilities.
“Probably the thing that is most frustrating is that not everybody around me perceives me the same way I perceive me. …I have to recognize that when I meet people and when I’m trying to establish relationships or friendships, the disability is always in the forefront of their mind.”
Ann Cody, Paralympic athlete (Portrait of Spirit, p. iv)
A New Eye on Disability: Atlanta, 1996
In 1996, the people of Atlanta experienced disability from a new vantage point, as Paralympic athletes from around the world navigated the city to participate in the 1996 Paralympic Games. Billy Howard and Maggie Holtzberg describe this event as being a catalyst in the creation of the Portrait of Spirit project, as the following excerpt from the introduction to their book explains:[/vc_column_text][vc_row_inner][vc_column_inner][vc_column_text]“This book came about, in part, because 1996 was the year Atlanta hosted the Centennial Olympic Games. Two weeks after the Olympics ended, the city welcomed the Paralympic Games, the ultimate competition for world-class, elite athletes with physical disabilities. Many of us were searching for ways in which to heighten the awareness of the Paralympic Games and seize the opportunity they offered to change able-bodied people’s perceptions of disability. A Cultural Paralympiad was envisioned, the first of its kind. …Paralympic athletes are not people who do well despite their physical limitations; they are people who do well, period. …It was with David Sampson that we began our work. As photographer and folklorist, we set out to gain an insider’s perspective. The hope was that nondisabled people would come to know people with disabilities, one story at a time.” (Portrait of Spirit, p. iv-v)
“Paralympic athletes are not people who do well despite their physical limitations; they are people who do well, period.”
25 Individual Stories, 1 Collective Voice
Howard and Holtzberg have an undeniable talent for capturing a person’s true essence. When collecting stories, they work to create a space where trust and self-expression run free; Portrait of Spirit is a testament to that talent. The 25 narratives offer moments of joy, sadness, resilience, and strength that can only be described as purely human. What follows is a glimpse at a few of these stories and the collective voice that rings out when stigma, biases, and preconceptions about people living with disabilities begin to fade.
“These individuals have fought long and hard about how they want to represent themselves to the nondisabled community. If there is a pattern to be discerned in their collective story, it is that they have succinctly reduced their lives to a personal story out of the necessity of defining themselves in a way that most of us do not have to.” (p. v)
Kate’s Story
“Cerebral palsy is a very different disability…it’s not socially acceptable yet. People don’t understand the movements…I say, ‘accept me.’ I’ve accepted myself.” (p. 87)

“Kate Gainer was one of 18 students to attend Atlanta’s first special education class for black children. It was an empowering experience for a black child growing up in a Southern segregated city. She says the most frustrating thing she went through as a teenager with cerebral palsy was that she couldn’t “strut” like the other girls could. Gainer’s intelligence, spunk and warmth have made her an invaluable advocate for people with a disability.”(p. 85)
Lauren’s Story
“I run into people who stop me on the street and speak very slowly or very loudly because they think because I am in a wheelchair that I have a mental disability. They do not expect that I can do the things I do…It’s a surprise to a lot of people.” (p. 66)
“Lauren McDevitt was ten when she experienced a muscle cramp in her thigh. She went to the school nurse to lie down. Within an hour, she lost all feeling and movement from her waist down. She captured a bronze medal at the 1996 Paralympic Games in dressage, a test of ability of rider and horse to communicate and work together through a series of complex moves.” (p. 65) Today, Lauren has earned her Master in Rehabilitation Psychology and Counseling degree, is married with two teenage boys, and is the Director of the North Carolina Office on Disability and Health.

Al’s Story
“I think everything finally came together when I started competing against other disabled people who were as competitive as I was. All of a sudden I had a group of people I could lean on and be a part of because they were athletes as well.” (p. 14)

“As a youngster, Al Mead lost his left leg above the knee due to circulatory problems. Mead has grown into the quintessential Paralympic athlete, whose excellence in competitive sport is equaled only by his commitment to increased awareness of the abilities of persons with a disability. He holds a U.S. high jump record at 1.73 meters. He set the world record for the long jump with a gold medal performance in the 1988 Paralympic Games in Seoul, Korea. Four years later in Barcelona, Mead won a silver medal in the long jump and sang at the closing ceremony.” (p. 12)
Catherine’s Story
“I would not attempt to do anything unless it was perfect. I believed I had used up my quota of failure. I had always thought this handicap was some colossal failure and I had used up my allotment of being imperfect.” (p. 36)
“Catherine Howett Smith is Associate Director of the Michael C. Carlos Museum at Emory University. A progressive neuromuscular disease began weakening her legs as a child. Reflecting on her journey coming to terms with her identity as disabled, she describes the importance of her role as a mother: ‘Throughout my life I had a lot of self-confidence because of intellectual gifts, but not physically because of my disability. Having my daughter was so profound, because it was the first time I did something physical—the ultimate physical experience. My self-identity is complicated—but with my daughter it is so simple—I am just Mommy.’ ” (p. 36)

Disability and Society: Looking Forward
When looking back over the past two decades, the progress our society has made since the 1996 Paralympic Games regarding disability seems obvious. The challenges faced by persons with disability may have become a bit less burdensome; a flicker of hope arises in the realization that society may finally be catching up with the extraordinary talents of this population. For many, however, there are new challenges and opportunities constantly arising as they continue to push forward. This perception of progress and its challenges looks different for each individual, as our stories and reasons for moving forward are unique and personal.
Encouraging members from both the disabled and nondisabled communities to come together to address issues of access, discrimination, and stigma that impact people living with disabilities is a critical step to jumpstarting change. “This book is not so much about the subject of ‘the disabled’ as it is about the cultural context in which disability occurs. That culture is shaped by the fact that we live in a society which is largely uninvested in the experience of being disabled. Despite the enactment of the Americans with Disabilities Act (ADA), physical and communicative barriers abound. Prejudicial attitudes towards people with disabilities are daunting.”(p. v-vi)
“…it is about the cultural context in which disability occurs.” “…we live in a society which is largely uninvested in the experience of being disabled.” (p. v-vi)
Interview with Billy Howard
In this interview, Howard describes his experience creating Portrait of Spirit: One Story at a Time, and reflects on the aspects of society that continue to present obstacles for people living with disabilities. He also weighs in on how he hopes Portrait of Spirit continues to serve as a resource for those in the rehabilitation community.
What was it like for you to create and be involved in this project?
Although I had been around people with disabilities since college, the experience of finding, meeting, listening to, and documenting the lives of the 25 people in this project inspired me, with their indominable spirit; shocked me, with the extraordinary efforts they were required to make in some cases just to get through their day in a world set up with obstacles the rest of us cannot fathom; angered me, with the loopholes that allow companies to discriminate against those with different abilities; and filled me with hope, through the stories of grace and pure will these individuals shared with us.
Did this project touch on any personal experiences for you?
This project was deeply personal to me. I attended St. Andrews College (now University) in North Carolina, which was one of, if not the first, barrier-free campus in the country, allowing people with physical disabilities to attend college with full access to classes and social activities. As a result, the campus was diverse not only along racial, ethnic, and religious factors, but also diverse in physical abilities. What I discovered at a time when I was coming of age, was that we all had different abilities and disabilities. I left St. Andrews with friends that informed my life as an adult.
What most surprised you about the experience?
Every documentary project is filled with the same surprise, and it is the thing that continues to motivate me to continue through a project’s obstacles and setbacks. That is the wonder and joy in having people share their most personal stories and reveal to us their challenges, pains, loves, and fears. Surprise may not be the right word in this case; it is more like awe.
Describe how you and Maggie worked together and influence each other.
I think what Maggie [Holtzberg] and I share in our work is an innate curiosity about humanity and a desire to discover and learn from people who have different experiences than us. Maggie shares that with others through her exceptional skills as an interviewer. When I was with her on interviews, I would sometimes leave forgetting that she had interviewed the subject; it had been more like witnessing an intimate conversation between very close friends. The revelations came from a trust she was able to build in a short amount of time. Some people were speaking of things that were deeply painful to them; Maggie gave them the confidence that their words would be honored and respected. I have tried to work the same way with the people who I photographed, making us a natural fit. I tried to take portraits that would honor the spirit of life they were revealing to us.
You have created many other projects that dive into this exploration of the human experience. How did this deep and genuine desire to know “the other” develop?
My alma mater, St. Andrews, was an introduction to people who I would have thought were very different from me and the beginning of a life-long discovery process that revealed the beauty in how we can learn, connect, and grow best by being around people that can bring us different perspectives. I have always sought out people, especially in my work, that bring me a broader understanding of the world through their different experiences.
What artist has most influenced your own work?
When I was in high school, I discovered the photography of Dennis Darling and saw how he used the camera as a ticket to explore the lives of people he never would have had access to without photography. Some of these were people with moral flaws, some were people in exotic locales, and some were heroes. The common denominators were a camera and curiosity. In a great act of serendipity, I was able to meet him and we became lifelong friends. He is still a mentor to me and my work.
How did this project impact how you view your own life?
It makes me profoundly thankful. I have had my own struggles with pain and illness (haven’t we all) including a form of arthritis that at times challenges the work I do. I have, quite literally, called on the strength of the people I met through this work, humbling myself with my own minor issues, and, as the Brits would say, carrying on.
In the 24 years since the birth of this project, how do you feel society has evolved (or not), and what needs to change?
While there have been many technological changes that have allowed people—through the use of computers and enhanced prosthetics, among others—to live life without as many obstacles, the loopholes within the Americans with Disabilities Act have also kept society from moving as fast as it should in breaking down the physical barriers to access for people with disabilities. We learned that firsthand recently as we went to a restaurant to celebrate the revival of our exhibit only to find multiple obstacles to those among us in wheelchairs that blocked access to the building.
How did you navigate that fine line between celebrating the “human spirit” and falling into the “super-crips” trap?
Our subjects made it very clear to us from the beginning that they didn’t see themselves as heroes, but merely people who lived life like the rest of us, but with more visually apparent hurdles. One of the people we included was former U.S. Senator Max Cleland, who lost one arm and both legs in a grenade mishap in Vietnam. He wrote a book, Strong at the Broken Places, which said that we all have injuries we need to heal, it’s just that with him and others with disabilities, those injuries are more visible. That philosophy is so powerful to me, basically saying we are all in this together, we must all have empathy with each other.
How do you think this exhibit impacts clinical care and rehabilitation science education?
I cannot imagine wanting a career in healthcare in any field without first having a deep sense of empathy for people, and particularly people whose lives can be improved through understanding, science, and medicine. My hope is to, through the interactions this project allows between the viewer and the people we photographed, create an enhanced understanding of how people in the medical/rehab fields process what they have learned and how they use their skills. Through Maggie’s interviews I hope it opens them to new ways to connect to their patients, and, hopefully, through my photography, they can look into the eyes of those they serve with a deeper desire to understand who they are as people. My desire would be for them to see the person first, not the disability. That makes all the difference.
How do you envision this book and exhibit moving forward through the rehabilitation community?
My deepest hope is that those on the service side are inspired by the voices of those in this work and gain a more profound sense of the beauty and nobility in the work they do and that those who are dealing with their own physical disabilities, especially those who are entering into this world for the first time, can see that they can live a full and wonderous life and that their disability will always be a lens through which they see it, but not the only one. They should never feel reduced by their disability, but lifted by their own humanity.
About the Authors of Portrait of Spirit: One Story at a Time
Billy Howard is a 2011-2012 Rosalynn Carter Fellow in Mental Health Journalism. He is the author of Epitaphs for the Living: Words and Images in the Time of AIDS; Portrait of Spirit: One Story at a Time, images and interviews of people with disabilities with an introduction by Christopher Reeve; and Angels and Monsters: A Child’s Eye View of Cancer with an introduction by Jeff Foxworthy. His photographs are in the permanent collections of The Library of Congress, the High Museum of Art, The Carter Presidential Center, and The Centers for Disease Control and Prevention. In a tribute to Dr. Martin Luther King, Jr., Howard’s photographs were projected on the stadium screen during the opening ceremonies of the 1996 Olympic Games in Atlanta, GA. His photographs are featured in the book Pandemic: Facing AIDS with an introduction by Kofi Anan, edited by Rory Kennedy. He received an Honorary Doctor of Literature Degree from St. Andrews University in North Carolina in 1996. Readers can learn more about Howard’s distinguished career here.
Maggie Holtzberg was the 2018 recipient of the American Folklore Society’s Benjamin A. Botkin Prize, recognizing her lifetime achievement in public folklore. She is currently the Manager of the Folk Arts & Heritage Program at the Massachusetts Cultural Council. As a folklorist, she works closely with traditional artists and communities through documentary fieldwork, grant programs and technical assistance. She has conducted field research throughout the state of Massachusetts documenting traditional arts, and established a traditional arts archive. She is the author of The Lost World of the Craft Printer (1992); Portrait of Spirit: One Story at a Time (1996); producer of the sound recording Georgia Folk: A Sampler of Traditional Sound (1990); and co-director/producer of the documentary film Gandy Dancers (1994). Holtzberg holds a PhD in Folklore and Folklife from the University of Pennsylvania and served as Folklife Program Director of the Georgia Council for the Arts prior to moving to Massachusetts.
![]()
This work is licensed under a Creative Commons Attribution 4.0 International License.
Molding a Crisis Curriculum
My initial instinct was to begin with the rich visual history of images depicting outbreaks of the plague from the Medieval and Renaissance periods to the activist art of the AIDS epidemic in the late 20th century, and apply art history skills—learning to read an image or object and analyze it within a social and historical context of its time. Confident that this was a great way for students to learn from the past to better understand our present situation, I began to prepare assignments that probed social and economic inequities of public health crises. I planned to start with a close reading of the chaotic scene of death of all social classes depicted in Pieter Bruegel the Elder’s painting, The Triumph of Death (1562) (Fig. 1) in relation to excerpts from Giovanni Boccaccio’s The Decameron (1351). In this text, Boccaccio described the relative privilege of the wealthy during the 14th-century plague in Florence, noting “the plight of the lower class and, perhaps, a large part of the middle class was even more pathetic,”1 as they did not have the means to leave the city and thus fell sick and died by the thousands. Breugel’s painting and Boccaccio’s text would then be discussed in relation to Nicholas Casey’s article, “College Made Them Feel Equal. The Virus Exposed How Unequal Their Lives Are,”2 to bring the discussion of economic disparities closer to home. Figure 1: Brueghel, Pieter the Elder (c. 1525-1569). The Triumph of Death. Ca. 1562. Oil on panel. 1.17 x 162m. Copyright of the image Museo Nacional del Prado / Art Resource, NY.
Additional opportunities for comparison to contemporary issues can be found in The Chronicles of Gilles Li Muisis, a 14th-century French manuscript chronicling Abbot Guilles li Muisis’ description of the plague in Tournai (modern-day Belgium). In this case, students would compare Pierart dou Tielt’s stark illustration (Fig. 2) of the city dealing with the problem of overflow and burial of dead bodies3 to contemporary photographs of mass burials across the world due to Covid-19 in Alan Taylor’s Vanity Fair article, “An Unimaginable Toll.”4
Figure 1: Brueghel, Pieter the Elder (c. 1525-1569). The Triumph of Death. Ca. 1562. Oil on panel. 1.17 x 162m. Copyright of the image Museo Nacional del Prado / Art Resource, NY.
Additional opportunities for comparison to contemporary issues can be found in The Chronicles of Gilles Li Muisis, a 14th-century French manuscript chronicling Abbot Guilles li Muisis’ description of the plague in Tournai (modern-day Belgium). In this case, students would compare Pierart dou Tielt’s stark illustration (Fig. 2) of the city dealing with the problem of overflow and burial of dead bodies3 to contemporary photographs of mass burials across the world due to Covid-19 in Alan Taylor’s Vanity Fair article, “An Unimaginable Toll.”4
 Figure 2: Miniature by Pierart dou Tielt,Chronicles ofGilles li Muisis (Tournai, c. 1353). The People of Tournai Bury Victims of the Black Death. ms. 13076-13077 fol. 24v. Bibliotheque royal de Belgique.
Another image from the same manuscript, called The Strasbourg Massacre (Fig. 3), highlights a brutal lesson from history—the desire of some groups to assign blame and malicious intent to the spread of the disease. In this case, Christians accused Jews of the purposeful spread of the plague by poisoning water sources, ultimately leading to the extermination of entire Jewish communities.5 While these images are painful to look at and learn about, they provoke compelling discussions on bigotry and intolerance when compared to contemporary conspiracy theories and overt racism toward Asian communities, particularly the Chinese, regarding the origin and spread of COVID-19. This is the power of art history; we can read about catastrophic events and the horrific failings of humankind, but seeing the images packs an emotional punch and promotes a profound reckoning of just how little human nature has changed. Learning to read these images critically and contextually gives students the knowledge and tools to challenge current social, racial, and economic disparities in our current pandemic.
Figure 2: Miniature by Pierart dou Tielt,Chronicles ofGilles li Muisis (Tournai, c. 1353). The People of Tournai Bury Victims of the Black Death. ms. 13076-13077 fol. 24v. Bibliotheque royal de Belgique.
Another image from the same manuscript, called The Strasbourg Massacre (Fig. 3), highlights a brutal lesson from history—the desire of some groups to assign blame and malicious intent to the spread of the disease. In this case, Christians accused Jews of the purposeful spread of the plague by poisoning water sources, ultimately leading to the extermination of entire Jewish communities.5 While these images are painful to look at and learn about, they provoke compelling discussions on bigotry and intolerance when compared to contemporary conspiracy theories and overt racism toward Asian communities, particularly the Chinese, regarding the origin and spread of COVID-19. This is the power of art history; we can read about catastrophic events and the horrific failings of humankind, but seeing the images packs an emotional punch and promotes a profound reckoning of just how little human nature has changed. Learning to read these images critically and contextually gives students the knowledge and tools to challenge current social, racial, and economic disparities in our current pandemic.
{kind=link}
 Figure 3: Miniature by Pierart dou Tielt,Chronicles ofGilles li Muisis (Tournai, c. 1353). The Strasbourg Massacre: Jews Burned to Death in Strasbourg during the Black Death, ms. 13076-13077 fol. 24v. Bibliotheque royal de Belgique.
Figure 3: Miniature by Pierart dou Tielt,Chronicles ofGilles li Muisis (Tournai, c. 1353). The Strasbourg Massacre: Jews Burned to Death in Strasbourg during the Black Death, ms. 13076-13077 fol. 24v. Bibliotheque royal de Belgique.
Choosing a Healing Approach
And yet, as I planned these new class sessions charged with critical comparisons to social and public health issues of the current COVID-19 crisis, I wasn’t prepared for how difficult it was to analyze graphic images of death, disease, and massacres, along with heartbreaking images of loss, sorrow, and mourning while living through an actual pandemic. I quickly realized that if the material was hard for me to digest in my own state of anxiety during the pandemic, I couldn’t impose this content upon my students. Recognizing certain methods would not serve my students at this time, I put aside my need to demonstrate the critical rigor of my discipline and revised the rest of the semester to focus on the study of art as a powerful instrument for healing, comfort, and joy. That said, I didn’t throw away my prior work; I will use this material in class at a less stressful time. In fact, after reflecting on the role of the humanities in recognizing the importance of dealing with the unknown, I decided to acknowledge my own uncertainties and share this experience with my students. In our first remote class, I told my students the story of my initial plans, showing them plague images as examples and described my plans to use these works of art to think critically about our current situation. I acknowledged my own struggle with the material and my decision to focus instead on the healing component of art. I shared that my course goals had shifted; I now wanted students to understand how art can provide healing, comfort, and humor in addition to illustrating the inequities of its time. With this in mind, I divided the remainder of the course into three modules on the following topics: Art and Personal Health, Art and Public Health, and Art in a Time of Crisis. As a health humanities scholar, I also applied some of Peterkin and Skorzewska’s key goals for health humanities in postgraduate medical education to this undergraduate course: providing a unique space to question, analyze, and critique contemporary practice while at the same time encouraging self-reflection and cultivating skills of reflexivity, in order to foster a greater understanding of the human condition.6 The following is a brief description and list of some resources used in these modules.Art and Personal Health
In this first section of the course, I assigned short and easily-accessible readings introducing the concepts and studies that demonstrate that looking at art and visiting an art museum benefits one’s physical health, mental health, and emotional intelligence. Students were asked to read and reflect upon these studies, and follow up with a “lab experiment”—a virtual visit to the Metropolitan Museum of Art’s (the MET) Temple of Dendur (via their MET360 project) in order to examine and reflect upon their personal response while viewing art in the midst of a pandemic lockdown. For most of my students (undergraduate non-majors, taking the course to fulfill a core requirement), this was the first time they heard of or even thought about these ideas connecting art and health. I knew I was on the right track when their written responses contained exclamations of surprise, wonder, requests for more information on certain studies, and an overall reaction of finding joy and peace while virtually wandering through the MET, a museum most had never visited in real life. Resources:- Why Going to an Art Museum Could Be as Good for You as Exercise
- Doctors to Prescribe Museum Visits in Pioneering Treatment
- Study Finds Med Students Who Make Time for Art Have More Empathy
- Researchers Have Found That Visiting Art Museums Can Offer Significant Relief for People Living With Dementia
- Visit NYC’s Metropolitan Museum of Art’s Egyptian Temple of Dendur via The Met 360
Art and Public Health
In this section, students investigated the connections between public art and public health. La Salle University in Philadelphia, PA is home to one of the most impressive mural arts programs in the country. We focused on Mural Arts Philadelphia (MAP) and their Porch Light initiative. Students considered Porch Light’s core message to “[work] closely with communities to uplift public art as an expression of community resilience and a vehicle of personal and community healing.”7 In a series of short, accessible readings and a video, students learned about the connection between public art and public health outcomes, and, more specifically, the effects of the Porch Light program on communities in Philadelphia. The Yale School of Medicine studied the impact and health outcomes in Porch Light communities and found increases in social cohesion and trust among neighbors, decreases in stigma toward individuals with mental health or substance-abuse issues, and an increase in the quality of the walking environment and perceptions of safety.7 After a written assignment reflecting on the connection between public murals to community health and wellness, students were asked to create their own “Art & Public Health Mural Arts Tour.” Using the Mural Arts Philadelphia website as their source, students created a PowerPoint tour with images, maps, and accompanying text, explaining why they picked a specific mural and how it related to community health and well-being. Their final slide involved a short critical thinking piece with the following prompts: How much did you know about Mural Arts Philadelphia before this assignment? How much did you know about Public Health concerns? Has this assignment changed the way you think about the role of city murals? Will you look at or interact with them differently? How so? Resources:- Public Art as Public Health
- The Porch Light Initiative Video – Community Healing Through Art
- Philadelphia Mural Arts: Porch Light Program
- Mural Arts Philadelphia website
Art in a Time of Crisis
Having set up an introductory framework on the research connecting art and health, the final summative assignment of the semester allowed students to apply what they learned to their own interests. This project was inspired by the phenomena happening in the creative world at that moment, where artists (and musicians, actors, writers, poets, etc.) were making their work public and free for all to provide joy, comfort, and entertainment during the global shutdown. The primary question of inquiry for this assignment was: what kind of creative work is being made and shared publicly right now while we are in lockdown and the world is reeling from fear, anxiety, and grief? Their task was to search their social-media communities to curate their own exhibition of art (defined in a broad sense) made in response to COVID-19 that offered some form of respite. The narrative accompanying their selections had to connect to the ideas and concepts discussed in the previous two modules with these prompts: Why did you select this creative work? How does this work of art relate to personal health, wellness, or public health? I shared my own list as a model for the assignment: Amplifier’s Free Downloadable art celebrating first responders and public health messages, The Getty Museum Challenge recreating famous works of art, Yo-Yo Ma’s Songs of Comfort, Lin Manuel Miranda & Andrew Lloyd Weber’s “Play-off” on Twitter, and Couple in Lockdown Create Tiny Art Museum for Their Gerbils, and noted that these examples in some way created a “biographic picture” of my interests and personality that I typically don’t get to share with students. Their exhibits were fabulous, with subjects ranging from street art, tattoos, video-game imagery, comics, poetry, songs, and concerts, to many funny and moving TikTok videos. The results were wonderful, and a joy to grade (a somewhat rare experience at the end of a semester).Reflections
This final project allowed me to get to know my students (and they me) on a level that would not have happened in the typical face-to-face classroom environment, which is contrary to traditional thinking about online teaching but makes sense when considering the nature of art. Sarah Blanton, Editor-in-Chief of JHR, noted in her Spring 2020 editorial that through art, “we find that connection of shared experiences, and perhaps we see each other a little more clearly, more compassionately.”8 This class made me rethink how I teach, and what I teach in the introductory course. The unexpected switch to remote teaching forced me to think about content and assessment in ways that I had not considered before. I struggled to leave behind traditional art history methods (visual analysis and critical social/historical studies) to embrace projects that involved studying art as “simply” a form of joy and comfort beneficial to one’s health. This resistance comes from a long history of art historians having to defend and explain the rigor and methods of the discipline to others, particularly in the medical humanities, where the arts can be pigeon-holed as a vehicle for empathy and therapy. I now realize my reluctance was limiting to myself, but more importantly, to my students. I found that there is time for both rigorous methods and compassionate, joyful pedagogy. As a result, these students left my class with more than the typical set of art history skills, just as I left class with a better set of teaching skills. It is Blanton’s idea of art as a method of seeing each other more compassionately that stays with me as I prepare for my Fall 2020 courses in light of the continuing pandemic and the additional public health crisis illuminated by the Black Lives Matter movement. I am planning modules for my students to engage with art critically, culturally, to have the difficult discussions, and to see each other more compassionately. Once again, I will use art as a means of addressing and interrogating issues of health and social injustice, using murals like Eric Okdeh’s The World to Come (Mural Arts Philadelphia, forthcoming, 2021) (Fig. 4) to encourage the trajectory of discussion, understanding, activism, and the ultimate goal: change. Figure 4: Eric Okdeh, The World to Come, (forthcoming Mural Arts Philadelphia, 2021) Eric Okdeh Instagram: @okdehmurals
Figure 4: Eric Okdeh, The World to Come, (forthcoming Mural Arts Philadelphia, 2021) Eric Okdeh Instagram: @okdehmurals 
![]()
This work is licensed under a Creative Commons Attribution 4.0 International License.
The development of rehabilitation medicine accelerated during and immediately after the First World War (WW1). The war’s unprecedented scale of casualties, in combination with an increased survival rate of the severely injured due to medical advances, left a high number of soldiers with both mutilated bodies and minds—and posed a major challenge to orthopaedic medicine at the time. Rehabilitation practices attracted increasing interest in Great Britain when the War Office requested support for soldiers to regain the highest possible level of functioning—to either return to the battlefields or, at least, to reintegrate as productive civilians back into society.1
The watercolor painting Physical Therapy at Bath War Hospital (Fig. 1), by the artist Sarah Elizabeth Roberts Horton (E. Horton), depicts one of the very first physiotherapy departments in England. The following analysis of this painting puts early developments in rehabilitation practices into historical context, in order to take a critical look at underlying principles of rehabilitation that are often taken for granted today. Using rehabilitation as the analytical point of departure provides a new way to see and understand this work of art.
The Painting: A Unique Historical Record

E. Horton’s painting is a unique record of one of the best-equipped rehabilitation facilities in a British war hospital during WWI. It depicts the interior of Q Block at Bath War Hospital in Bath, South West England—near Bristol—where injured soldiers received applications of massage, mechanotherapy, electrotherapy, hydrotherapy, and light therapy. According to the label attached to the front of the frame, “2162 patients have been treated and 49305 treatments given” since the hospital’s opening in November 1916 until its closing in September 1918.2 The Wellcome Trust Library in London, UK, now holds the original painting (50 x 73.6 cm).
The Artist
Sarah Elizabeth (Ettie) Horton (E. Horton) (1862-1959), the artist who had the keen insight to paint Physical Therapy at Bath War Hospital, was born in Australia of English parents. Her father was a mining engineer; her mother died when she was 11 years old. Horton was sent to England, where she was brought up by an aunt, received education, and became an artist. Horton established herself as an artist in London and moved later to Bath.3 She specialized in architectural watercolors of Bath and other towns; and, later in life, developed expertise working with gesso (a white paint base to prepare surfaces for paint). Horton’s work was regularly seen at exhibitions at the Bath Society of Artists; she also had paintings accepted for exhibitions at the Royal Academy and the Royal Institute of Painters.4 The Victoria Art Gallery in Bath currently holds 13 of Horton’s watercolors. The Watchman’s Box, Norfolk Crescent, Bath (Fig.2) is typical of her work.

Analysis From a Rehabilitation Perspective
My initial viewing of the painting, Physical Therapy at Bath War Hospital, was through the eyes of a curious maverick with a professional background in both medical anthropology and physiotherapy. In my day job, I facilitate knowledge exchange between rehabilitation practitioners and their patients to support critical reflection and change in clinical practice. This explains my somewhat different point of departure compared to an art historian who would traditionally begin the research with a focus on objects and aesthetic principles.
At first, I was puzzled by the considerable difference between this painting and the artist’s architectural paintings that make up her body of work. Curious to find any hints as to what might have motivated Horton to paint one of the first physiotherapy departments in Britain, I tried to understand who she was as a person—including her social circumstances and life in Bath.
Secondly, my background in medical anthropology sparked my interest in investigating conceptualizations of healing and the body. I was intrigued to learn about the everyday experiences of those working in the Q Block and their patients, and how these experiences related to the wider social and political context of that time.
Thirdly, my current role as facilitator of change in rehabilitation urges me to think practically, which motivated me to explore what the history of rehabilitation can reveal about issues related to how rehabilitation is practiced today.
In this article, I show how these three points are related. I demonstrate that rehabilitation practices are socially situated, and that the concept of rehabilitation, with its origins in war medicine, is of a highly political nature.
Bath War Hospital
The back of the painting (Fig. 3) provided a clue worth tracking down in my quest to figure out the artist’s motive for capturing this moment at Bath War Hospital. At the very top of the reverse side of the image are three photos stuck onto the frame, titled: Whirlpool Bath Room, Exterior of Q Block, and Radiant Heat Room. Below them are 13 workshop drawings of gymnasium equipment with the following descriptions: Rotation of shoulder joint; Attachable belt for stretching contracted hamstrings; Flexion and extension of knee; Rotation of wrist joint; Flexion and extension of fingers; The saddle crutch; Slings for attachment to any form of crutch (2x); Exercise for weak thumb and fingers; Ankle rotation; Flexion and extension of the ankle; Flexion and extension of elbow joint; and Pylons.

Local newspaper articles from the period during and after the war offer insight into the possible source of the workshop drawings and photos, but also shed light on the social and political circumstances around the establishment of the hospital’s Q Block.
Bath had a longstanding reputation for innovative medical treatments, including hydrotherapy.5 The town’s geographical positioning and railway connections to the South coast were also ideal to transport convoys of wounded and sick soldiers from the British Expeditionary Force to the town for treatment. Due to a shortage of medical and nursing staff in the British army, the War Office was in need of civilian practitioners.1 In May 2015, the Mayor of Bath received a telegram from the War Office to provide additional hospital accommodation for wounded soldiers. After consulting with Bath hospital authorities, a committee was formed to negotiate with the War Office.6 The War Office agreed to fund the basic infrastructure of a new hospital, while the costs for its upkeep, and for more specialized and advanced facilities, were to be funded locally through volunteers and donations from residents.7
A local businessman, Alderman Cedric Chivers, paid for the entire cost of the building that became known as the Q Block, and sponsored the electrical and mechanical equipment inside it. Most of the appliances were manufactured by local engineers in Bath.8 The Bath Surgical Requisites Association, supported by 290 volunteers and temporarily housed in Chiver’s premises near the hospital, made many appliances for injured soldiers, including artificial limbs.9 The workshop drawings that are stuck to the reverse of the frame might be copies of drawings used in the Association’s workshops. Bath War Hospital was a local initiative, which makes it less surprising to find this painting in the body of art from a local artist who was concerned with motifs representing the town.
The hospital was opened in April 1916—the Q Block in November 1916. When the management transferred from the Ministry of War to the Ministry of Pensions, the facility was renamed the Bath Ministry of Pensions Hospital in 1919; it closed in 1930.10 Local journalists were only allowed to enter the facility after 1918. In March 1919, a local newspaper published four photos illustrating orthopaedic treatment carried out in the former Bath War Hospital.11
A Rehabilitative Moment Frozen in Time
The scene depicted in the left section of Horton’s painting, featuring a man exercising with a sculling apparatus in the front, a person on an exercise bike directly behind, and two men using mechanical handles fixed to the wall for forearm rotation, is almost identical with one of the published photos. The depiction of the masseuse in the center of the painting is remarkably similar to a masseuse in another photo; even the clock in the center back of the painting resembles the clock in the photo. These images served the artist most likely as models.
Since Horton could have only had access to the images after the end of the war, the painting came most likely into being in 1919 or later. Whether the three photos stuck to the back of the painting are part of the same series of images published in the newspaper is unclear. While the workshop drawings titled Flexion and extension ankle, and Flexion and extension of fingers resemble the images on the right side of the painting, it is possible that a previous owner or commissioner rather than Horton added them to the frame. This person probably had close links to the hospital, and also attached the label to the front of the wooden picture frame that honors J.Y.W. Macalister, Esq.— the Secretary and librarian of the Royal Society of Medicine who suggested investing in the electrical and mechanical equipment—and the donor of that equipment, Cedric Chivers.
Hospital as Military Machine
Horton’s painting depicts a spacious room with high ceilings and three large windows. The room serves as a physical therapy department for wounded soldiers, and holds electrotherapy equipment, whirlpool baths, mechanical exercise machines, and therapy beds. The main conditions treated in the Q Block were “wasted muscles, stiff joints, painful scars, in consequences of injuries received,” shell shock, and trench foot.12
Five men at the right side, two men at the left, and two at the center back of the image exercise using mechanical exercise machines. In the center, a masseuse mobilizes the hip and knee of a man lying on a therapy bed; behind her stands another woman in nursing uniform who seems to support a man using one of the mechanical exercise machines. Three men, seated in the back center left of the picture, wait for their turn. They appear engaged in activities even while they wait. One is depicted reading, and one is looking into the center of the room with a booklet on his lap; the third is half hidden behind a dividing wall.
Behind the therapy bed in the center right, a man is seated with his arm in a whirlpool bath resembling the bath in one of the photographs stuck to the back of the painting. On the wall to the right is a panel for control of magnitude and type of electric current. Most of the men are fully dressed wearing blue suits, white shirts, and red ties. War and military hospitals provided recovering soldiers in Britain with these blue, often ill-fitted, hospital suits that became known as “hospital blues.”13 The uniforms identify the men in the painting as soldiers still subject to military discipline, and give a sense of institutionalization. The following lines from a poem written by a soldier for the hospital’s magazine that was published by the soldiers themselves, confirms this reality:
When the M.O. makes a visit,
Silence! Do not make a din,
Keep the bedclothes nice and tidy –
All the ends tucked nicely in;
Keep your locker neat and shining,
Don’t drop paper on the floor,
When you get your daily ration,
Do not ask for any more.14
The male figure facing the viewer in the middle right section of the painting is Dr. King Martyn, the physician in charge. He overlooks the application of light therapy for a man who seems so severely injured that two nurses are needed to carry out the treatment—one to prop him up on a chair and the other to apply the bath. A dominant vertical post frames the scene.
Dr. Martyn considered good treatment outcomes for wounded soldiers as “being able either to rejoin their units or perform munition or other work.”12 These therapy aims reflected the then overriding military agenda of rehabilitation. The increase in the number of wounded soldiers leading up to 1916 encouraged the War Office to boost investment in therapies that promised to restore function in wounded bodies, enabling men to either re-join the military forces or find long-term employment as civilians.13 Bath War Hospital was built as a result of this additional investment.
Dr. Martyn lamented “the shell-shock element producing the unconscious malingerer, and by the fact that whereas the civilian is, as a rule, most anxious to get back to his work, many of these poor soldiers do not, or cannot, co-operate with the physician.”12 His ideas about the necessity of active engagement in therapy stood in sharp contrast to the soldiers’ common belief in well-deserved rest.13
Horton’s watercolor serves as a visual record of the entanglement of medicine in warfare, which was also a concern in the local media at the time. Critical voices associated the rehabilitation provided in the Q Block with war politics: the “war hospital was under war office control and the war office was essentially a military machine.”15
Masculinity in Crisis
Advancements in technology had paved the way for modern industrial warfare, causing devastation and violence of unprecedented scale during WW1. Technologies producing injury and death rather than improvements seemed a huge setback for modern life often defined by “development” and “progress.” Mutilated male bodies and shell shock exacerbated long-held concerns of mental and physical degeneration.16 Alongside economic and social upheavals,17 fears about racial degeneration and a decline of heroic manliness—which was thought to be needed to fulfill imperial purposes—appeared to shatter the dream of the British Empire. Medicine had long contributed its part to these public debates by advocating for compulsory military training and health programs for the poor to ensure adequate manpower for the army.18 The emphasis on normative heroic ideals of manliness through militarized medicine at Bath War Hospital is evident from another verse of Ellerton’s poem:
You must shave before nine-thirty –
You’ve an awful dirty face;
Visitors will soon be coming,
Please do not be a disgrace:
When you get your daily dressings,
Just be silent as you can,
Do not jump if it should hurt you,
Be a soldier, be a man!!14
Here, the nurse questions his masculinity should he disregard her standards of cleanliness and openly express pain. Her expectations of manliness represent regulations from eighteenth-century hygiene movements and a Victorian and Edwardian ideal of masculinity defined by military heroism.18 This poem illustrates how wounded soldiers struggled with the incompatibility between social expectations of manliness and their physical and mental injuries.16
While medical agendas shaped normative ideals in society, the very same ideals informed the culture of medicine. Medicine had, historically, allied itself, for the most part, with the military as a means to gain recognition as a profession and to preserve medicine as a male domain. As a result, medical practice followed a masculinized vision of medicine based on values framed in military language—such as active, brave, and courageous.18
A Painter’s Statement
Horton, however, puts two women wearing nursing uniforms into a central position in her painting. The woman who mobilizes a soldier’s leg in the foreground of the picture is the chief nurse and masseuse Marjorie Cook. Her expertise in electro-mechanical therapy—and her adaptations to electrical appliances that helped optimize their effects—were regarded highly in Bath.8 The depiction of Cook and the men she is treating in the painting is identical with a photo from inside the Q Block published in a local newspaper. The journalist describes the image as follows: “the sister-in-charge (Miss M. Cook, A.R.R.C.) is shown exercising the patient’s weak leg.”11 The photo and the artist represent Cook as active, while the man lies in a passive position. The image challenges traditional power relations by contradicting the notion of Victorian masculinity, according to which the attributes active and strong are associated with men, while women are considered passive and weak.18
By placing two women at the center of the painting, Horton presents them as having a pivotal role in war medicine, which contradicts more common views of the nursing discipline as a profession of considerably lower social status than the higher (male-dominated) stratas of medicine. The image suggests that expanding their expertise in new therapy methods that restore the physical functioning of soldiers enabled them to secure a higher reputation by acting more “man-like,” highlighting their invaluable contribution to the war. The image can, therefore, be perceived as a feminist painting.
Building a Modern Future on Classical Ideals
The vast number of wounded soldiers in WW1 accelerated the development of new rehabilitation methods.1 The most pressing issue at the time, besides finding pragmatic solutions to overcome the tremendous human suffering caused by industrial warfare, was the need to identify ideals for a better future. Common concerns about racial degeneration and the decline of masculinity prepared the ground for a return to ancient Greek beauty ideals of the male body that seemed a promising response to the desire to reconstruct the wholeness of bodies and restore stability in society.16 Horton’s painting of the Q Block at Bath War Hospital embodies these very ideals for a better future and reveals how gender concepts framed early developments in rehabilitation, particularly the newly emerging discipline that is known as physiotherapy today.
Horton’s use of muted, warm colors creates a harmonious effect. All the attending professionals are bathed in sunlight coming in from the large windows, as if the war had never happened. The sunlight coming through the windows is perhaps a visual reference to healing attributed to the three natural remedies of air, sunlight, and water—a concept that originated in the Alps and found supporters among the British middle-class in the years leading up to WW1.5 The electrical appliance for light therapy to the right in front of the doctor was a modern way of extending this approach.
Applying natural remedies from outside the body, as opposed to relying on the therapeutic effects of intervening inside the body, have been popular in Greece, Rome, and other parts of the world since ancient times.5 In keeping with the classical ideal of harmony, the aim of these physical therapies was to reconcile tension between body and mind. The focus on the person as a whole made the application of these therapy forms attractive for the treatment of soldiers with permanent injuries, since the medical emphasis on improving the function of individual body parts failed to deliver satisfying outcomes.16
European Innovations
In European towns where medical doctors had a strong influence on the spa culture, a systematic approach to physical therapies that included a combination of bathing, electrotherapy, exercising, and massage had become part of the treatment provided in hospitals by the end of the 19th century. In the 1880s, the British Medical Journal (BMJ) began to publish articles on the clinical effectiveness of massage; hospitals across Great Britain employed an increasing number of masseuses. The first masseuses were nurses who completed additional training provided by physicians or senior masseuses at mainly London-based training schools.
In 1895, the Society of Trained Masseuses was formed as a branch of the Midwives’ Institute and Trained Nurses’ Club. This organization was the precursor of the Incorporate Society of Trained Masseuses (1900), the Chartered Society of Massage and Medical Gymnastics (1920), and the still-existing Chartered Society of Physiotherapy (1944). While early members were predominantly nurses, an increasing number of women began to take up massage—including the application of various physical therapies—as a career on its own. Electrotherapy became increasingly popular to treat symptoms attributed to nervous ailments, which were believed to be a side-effect of industrialization and modern life. During the war years, the scope of its application broadened rapidly to include, for instance, testing and stimulating muscles.5
Advances in exercise programs and massage therapy were strongly influenced by the “movement cure” developed by the Swedish physical educator Dr. Pehr Henrik Ling, who distinguished between active movements encountering resistance and passive movements performed on the body, such as rubbing—a precursor to massage. Swedish physician Dr. Jonas Gustaf Wilhelm Zander took Ling’s approach a step further by developing the first mechanical equipment to control the exact weight-resistance needed to optimize development of individual muscles. He created gymnastic appliances for different movements; his equipment collections became internationally known as Zander Institutes.19 Bath War Hospital was one of the few hospitals in Britain in possession of an almost complete Zander Institute.12 Some of these machines are shown in the painting.
Innovation at Bath War Hospital
Many soldiers came to Bath War Hospital with severe injuries that caused muscle weakness and limited mobility. Zander machines enabled them to gradually improve their physical strength and range of movement, easing the transition to outdoor team sports, which were closely connected to national identity in Britain and believed to reconnect soldiers with their civilian lives.1 Dr. Martyn said the participation in regular sport activities at Bath War Hospital “give[s] free play to the arm and shoulder muscles” and noted the soldiers’ willingness to get involved.12 The hospital also organized annual public sports contests for patients and staff, which were attended by large crowds of Bath citizens.20
The painting helps viewers see early developments in rehabilitation as attempts to restore damaged masculinity through providing opportunities for men to get active and rebuild their physical strength. Horton depicts all soldiers, including those waiting for their turn, as engaged, which contradicts Dr. Martyn’s perception of uncooperative patients.12 In so doing, Horton creates an idealized version of soldiers recovering from injuries during WW1, which bears a certain resemblance to ancient Greek sculptures that represent male bodies as physically strong and in motion.21 Both active and passive movements helped to heal the body and mind as “muscles became markers of men’s rehabilitation and civilian reintegration, showing that the fragmented man could be restored through classical ideals of wholeness.”16
The similarities between the photos published in the local newspaper and the painting reveal the meticulous care the artist took to achieve a realistic representation of the electrical and mechanical equipment in use at the hospital. While her quest for realism represents classical ideals, the painting itself shows the potential of technology to heal as opposed to causing destruction and violence. Here, reconstructing the body is aligned with modernity.22 During the war, the Q Block and its then state-of-the art equipment, received many visits from respected experts—and royalty, including King George V and Queen Mary, who were impressed with the innovative treatments provided.6 The artist merges classical and modern values to create aesthetics of movement that counteract the brutal reality of warfare and turn efforts to restore the male body into a symbol for healing the nation.16
Rehabilitation as Sacrifice
Horton painted the soldiers’ uniforms in a strikingly strong blue, perhaps identifying them as “Tommies”—patriotic heroes. The image of recovering soldiers actively exercising or having their limbs exercised by masseuses draws attention to their resilience as well as to their weakness and, ultimately, to their continuing sacrifice for the nation. Horton’s painting combines imagery of passive movement with heroic images that hide any form of strain or discomfort. The facial expressions of all figures in the image are shown in an emotionally neutral way, which idealizes the beauty of restoring and re-activating the male body. The image can be interpreted as an example of attempts at the time to re-evaluate endurance as courageous, softening the concept of heroism without posing a serious challenge to the normative masculine ideal.23 In so doing, Horton contributes to the nation’s collective memory of overcoming devastation by returning to classical ideals of the male body.
At the same time, the imagery of heroic sacrifice provides meaning to the suffering not depicted in the painting. Many soldiers admitted to the hospital were, for instance, Australians with little or no previous connection to the residents of Bath.10 The hospital, however, only existed due to the remarkable efforts of local residents who funded, equipped, and staffed it following an appeal to the public that read, “…local help must supply these men, who have sacrificed themselves for their country.”7 Many local people sacrificed their own health as a result. Although Bath War Hospital was one of the best equipped hospitals in the country,8 the Royal United Hospital in Bath lacked resources to provide the most basic care to the general public.24 The remarkable achievement of establishing one of the best rehabilitation facilities in the country came at considerable cost to the local population. The civilian contribution to Bath War Hospital was, nevertheless, a chance for civilians to become heroes themselves. A review of the hospital’s history in the local media at the time reads: “The Combe Park Institution…has had associated with it a degree of self-sacrifice and enthusiastic, sustained voluntary service by almost every class of the community that has not been equalled within living memory.”10 The many civilian volunteer hospitals across the country enabled civilians to contribute to the war efforts, which made medicine—with its newly developing specialization to help reconstruct soldier’s bodies—a main driver behind mobilizing the whole nation for war.13
Rehabilitation as a Means to ‘Return to Order’
Horton’s painting is part of a wider societal trend throughout the western world of reviving classicism as a form of expression and guidance for modern life at the beginning of the 20th century. The French artist and poet Jean Cocteau is believed to have coined the term, “return to order” (retour à l’ordre), which has become widely used to describe the European art movement following WW1.25 Avant-garde artists such as Georges Braque and Pablo Picasso returned to forms of realism and classicism as an artistic means to restore a sense of reassurance in times dominated by feelings of distress in the aftermath of WW1.26 Greek ideals of masculine beauty manifested in the numerous war memorials erected across Britain. The notion of heroic self-sacrifice helped to make the irreparable harm industrial warfare had done to body, mind, and civil life more bearable and meaningful. At the same time, the idealized active and reconstructed male body helped to put an end to the devastation by rendering individual suffering invisible, thereby avoiding the feared decline in masculinity.16 Horton’s painting and its aesthetics of movement can be understood as an early form of images depicting what Carden-Coyne calls “healing aesthetics,”16 in which male beauty is defined as white – marble – muscular. Idealized imagery of such bodies intended to help the nation as a whole come to terms with the consequences of the war and reconstruct a civilization thought to be lost.
Conclusion
Early developments in rehabilitation, particularly physiotherapy, took place against this background of war and recovery. Due to medicine’s strong entanglement with the military, rehabilitation as practice helped to mobilize the nation for war. It was mainly grounded in a masculinized vision of medicine framed around activity, courage, and bravery, as opposed to domestic values such as peace, compassion, and care.18 The return to classical forms of the male body in art further reinforced the paradigm of normalization in accordance with stereotypes of manhood—which helped promote physical rehabilitation as an emerging discipline. Physical Therapy at Bath War Hospital urges us to take a closer look at how political developments and social expectations have informed rehabilitation practices.
The author wishes to thank Dr. Francis Duck for being so generous in sharing his historical resources and knowledge about Bath War Hospital. A big thanks is offered as well to Jon Benington, manager at Victoria Art Gallery, for his useful guidance.

![]()
This work is licensed under a Creative Commons Attribution 4.0 International License.